
Commentary|Podcasts|April 30, 2026
NeuroOp Guru: When eye and brain strokes point to antiphospholipid syndrome
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, discuss how eye and brain vascular events such as retinal vein occlusion and stroke can signal antiphospholipid syndrome and require further evaluation.
Advertisement








In this latest episode of the
Lee is the chair of the Blanton Eye Institute at Houston Methodist Hospital and a professor of ophthalmology, neurology, and neurosurgery at the Weill Cornell Medical College. Carey is the Neil R. Miller Rising Professor of Ophthalmology in the division of neuro-ophthalmology with the
Carey outlined the
Concurrent arterial and venous events should raise suspicion for systemic disease
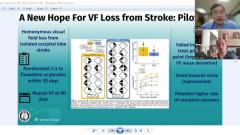
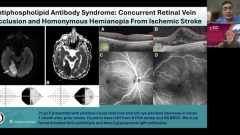
The discussion centered on a 71-year-old patient who presented with a homonymous hemianopsia from a posterior cerebral artery stroke and later developed a retinal vein occlusion with decreased visual acuity. Carey emphasized that this combination—visual field loss localizing to the brain alongside monocular vision loss—signals involvement of both central nervous system and ocular processes, prompting consideration of a unifying systemic cause.
Although common vascular risk factors such as hypertension can contribute to both stroke and retinal vein occlusion, the temporal proximity and involvement of both arterial and venous systems should raise concern for an underlying hypercoagulable state. Antiphospholipid antibody syndrome is high on the differential diagnosis in such cases, particularly when events occur across different vascular beds.
The conversation also addressed multidisciplinary management. Depending on associated systemic features, patients may require evaluation by hematology for anticoagulation and by rheumatology if an underlying autoimmune condition, such as systemic lupus erythematosus, is suspected. Additional therapies, including hydroxychloroquine, may be considered in patients with autoimmune disease to reduce thrombotic risk.
Carey concluded with a key clinical takeaway: when patients present with both arterial and venous occlusions, clinicians should look beyond typical vascular risk factors and pursue further workup for hypercoagulability or cardiac sources. Early recognition is essential, as appropriate treatment can reduce the risk of recurrent thrombotic events, including stroke.
Reference
Yu HJ, Karimaghaei C, Nguyen TA, et al. Antiphospholipid antibody syndrome: concurrent retinal vein occlusion and homonymous hemianopia from ischemic stroke. J Neuroophthalmol. 2025;45(4):e275-e277. doi:10.1097/WNO.0000000000002289
Advertisement
Related Content
Advertisement




Latest CME




















Advertisement
Advertisement