
Opinion|Videos|September 21, 2023
NeuroOp Guru: Visual outcomes in solid versus cystic pituitary adenomas
Author(s)Andrew Carey, MD, Andrew G. Lee, MD
Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss visual outcomes in solid versus cystic pituitary adenomas.
Advertisement








Video Transcript
Editor's note - This transcript has been edited for clarity.
Andy Lee, MD:
Hello, and welcome to another edition of the NeuroOp Guru. I'm here with my good friend, Dr. Drew Carey. Hi, Dr. Carey.
Drew Carey, MD:
Hi, Dr. Lee.
Andy Lee, MD:
And today we're going to be talking about visual outcomes in solid versus cystic pituitary adenoma. Drew, maybe you could just give the audience an idea of why does this even matter? Why should we even care?
Drew Carey, MD:
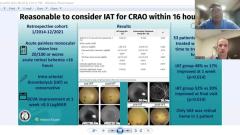
That's a great question, Andy. You know, I think we're all familiar with pituitary adenomas, and they grow and they can compress the optic chiasm and cause visual field loss, and severe visual disability. Most patients have visual recovery when we do a resection as long as it's not too late. They're not too pale, their vision loss isn't too far gone. But, um, you know, not everybody has full recovery. And I don't think we have a really great understanding of why some patients have better recovery and other patients don't. And sometimes we see patients with giant pituitary adenomas, and their vision is surprisingly really good or even normal. And so I think trying to understand what factors may play a role in vision loss and vision recoveries is helpful for prognosticating with the patient and telling the neurosurgeon how urgent do they need to have surgery? Like, do they need to have it 5 years ago? Or do they need to have it like today or tomorrow? Or is it okay to do it in a month or 6 months or something? And so I think, you know, trying to help elucidate those factors, which are not entirely clear, is a worthwhile research investigation.
Andy Lee, MD:
And so what did they do in this study in terms of cystic versus solid tumors?
Drew Carey, MD:
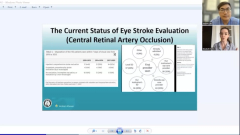
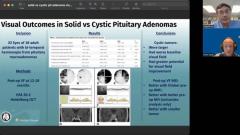
Yeah, so this was a retrospective review, they looked at all their patients who had visual field loss and had transsphenoidal resections, and had pathology confirming pituitary adenomas, and they identified 32 eyes from 18 patients, because some of the eyes did not have a bitemporal hemianopia or, like, you know, if they had a total scotoma that eye was excluded. And they separated into patients who had cystic components based on MRI imaging, and those that were solid only. And they looked at their post-op visual fields at somewhere between 12 and 18 months out and all the patients got an automated visual field with a 30-2 protocol and they used the Heidelberg OCT to look at structural changes.
Andy Lee, MD:
And what were the results?
Drew Carey, MD:
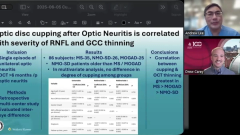
Yes, so they noticed that patients with cystic tumors tended to be larger, and that patients with larger tumors tended to have a worse baseline visual field and had more visual field recovery, which probably makes sense. As long as you're not too blind, you have more room for improvement. And they noted that, you know, some of the cystic patients had really large tumors. So they did a subset analysis when they removed those and the big things that seem to impact visual recovery, were patients who had a thicker pre-op or RNFL OCT, tended to be better meaning, you know, they probably had more of their optic nerve left. And patients who had a better pre-op, visual field by mean deviation had a better post-op mean deviation, meaning they hadn't lost as much vision. And that was on a univariate analysis, but didn't hold up on their multivariate, and patients with smaller tumors had better post-op visual fields, meaning, you know, the tumor hadn't grown as large, it probably hadn't been compressing the optic chiasm as long and had probably put less strain on the visual fields, or on the optic chiasm and less strain, therefore, on the vision. And the patients with cystic tumors did have worse mean deviations like minus 17, essentially, compared to minus 5, on average. And they did have a bigger change with those patients with cystic tumors improving almost 9 decibels compared to only .2 in the solid group. But again, there's probably a big factor cross playing there. And then the tumor diameters were much larger in the cystic patients where they were, on average 31 millimeters compared to 23 millimeters. So again, and perhaps it's that these cystic tumors can grow more rapidly because they don't have to have tumor doubling to grow, they have this cystic component, and that that rapid change may portend, you know, of more stress strain on the optic chiasm and more visual field loss. But the good news is most of the patients had pretty significant recovery, whether they were cystic or solid and that had good improvement in vision.
Andy Lee, MD:
And what kind of OCT nerve fiber layer do you kind of use as a cut off for patients when you tell them, hey, you're gonna get your vision back, or maybe you're not gonna get your vision back? Or do you think you can even use the number like that nerve fiber layer thickness?
Drew Carey, MD:
I don't have an exact cutoff. I know some people, you know, even before we were using an OCT was kind of, you know, if if you had an optic nerve that looked like aspirin tablet, you probably weren't getting your vision back. You know, if there's pretty marked paleness, it's not great. I know, you know, there are some studies that have given a cutoff on the RNFL. And I don't think it's like an exact, you know, it's not, it's not a highly specific, it's kind of, you know, if you have a really good RNLF, like you're in the 80-100, you're, you're probably going to come back with what looks like a normal field on on a 30-2 or 24-2 and using a size 3 stimulus. And if you know if you're under 60, probably not so great. But I don't have a hard cutoff. And I think what's really fascinating is kind of the ganglion cell, I think if you're, you know, if you have, you know, total ganglion cell wipe out, that doesn't look like a homogenous, you know, defect or not a vertical defect, then you're probably not going to have good vision afterwards. Some patients will have really, you know, severe binasal thinning on their ganglion cell and still have really good vision recovery, which is still a little bit of a mystery. I don't know how they're seeing a temporal field without any ganglion cells, but it happens.
Andy Lee, MD:
Yeah, I'm always very cautious for ophthalmoscopic appearance of the nerve. And OCT, I say, look, we're hoping for the best, but we have to be prepared for the worst and you're in the green zone that makes it more likely that you're gonna get your vision back. You're in the yellow zone, it's borderline. Red zone, we're trying to keep what we have not really gain back what we lost, but we'll take what you get. And I've been shocked, people in the red zone, they just got better. So I never say never anymore.
Drew Carey, MD:
Yeah, which is cool. And hopefully we'll find some new protective factors in the future. I think when you're in the red zone, you got to bring out that red zone defense and you definitely want to protect.
Andy Lee, MD:
So what do you think the take home messages for the general ophthalmologist listening to today's NeuroOp Guru?
Drew Carey, MD:
Sure, for the general ophthalmologist, you know, I think if you have a neurosurgeon or [inaudible] who you know is referring your patient for baseline vision evaluation, and you see a cystic tumor. And they have, you know, a very mild visual field defect and said, Oh, it's not that bad. We could probably watch this, I think it's important to be wary that the cystic tumors may grow a lot faster than our solid tumors. They don't obey the tumor doubling time law. And those patients may have rapid vision loss from rapid growth, and that may portend a worse visual prognosis. So I think that's probably the main take home point is watch out for cystic tumors. The good news is a lot of them will have visual recovery, but not always.
Andy Lee, MD:
Well, that's really great. Dr. Carey as always, thank you for your time. And that concludes yet another edition of the NeuroOp Guru.
Drew Carey, MD:
Always a pleasure.
Advertisement
Related Content
Advertisement




Latest CME






















Advertisement
Advertisement