
|Videos|September 29, 2022
NeuroOp Guru: Pearls about the diagnosis, treatment of visual snow syndrome
On this week's episode of the NeuroOp Guru, Andy Lee, MD, and Elizabeth Fortin, MD, discuss visual snow syndrome and whether it should be evaluated during standard in-clinic ophthalmologic testing.
Advertisement








This transcript has been lightly edited for clarity:
Andy Lee, MD:
Hello, and welcome again to the NeuroOp Guru. I'm here with my good friend Elizabeth Fortin, MD. Hi, Elizabeth.
Elizabeth Fortin, MD:
Hi.
Andy Lee, MD
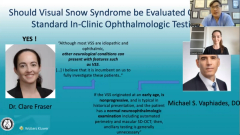
And today we're going to be talking about a recent article. Should visual snow syndrome have any evaluation outside of standard in clinic ophthalmologic testing? The two participants were Claire Fraser, MD, and Michael S. Vaphiades, DO. Elizabeth, maybe you could just tell us what is visual snow.
Elizabeth Fortin, MD:
Visual snow syndrome is an array of symptoms that we see in people who describe having small flecks or dots in their visual field. So normally, it is black and white dots all over the visual field. It's often described as a TV that's out of tune, like an old TV. And it persists over time. So it has to be at least 3 months to call it visual snow syndrome. And it's often associated with other visual symptoms such as photophobia, or other and topic visual phenomena.
Andy Lee, MD:
And their exams are normal?
Elizabeth Fortin, MD:
Yeah, so the people who we call the primary visual snow syndrome have a completely normal examination. They often describe the symptoms that I just talked about, in a very classic way. They don't have any other neurological symptoms, and their exam is completely normal, as opposed to people who have, for example, secondary visual snow, which can have other symptoms or other findings on exam.
Andy Lee, MD:
So you agree that we should do a visual field, automated perimetry and a macular OCT on all of these people?
Elizabeth Fortin, MD:
Of course, you have to perform a complete eye exam, including a dilated fundus exam, I believe. And in clinic in the office, it is easy to obtain an macular OCT to assess the retinal layers. Most importantly, probably the outer retinal layers in the visual field testing we should have done in all those people.
Andy Lee, MD:
And have you ever found anything on these people?
Elizabeth Fortin, MD:
It is very rare. If you do a good exam, questionnaire or history with these people, and then really don't have any other symptoms exist, it's extremely rare to find other findings on your exam, but it can definitely happen. But I would say it's pretty rare. Have you found any?
Andy Lee, MD:
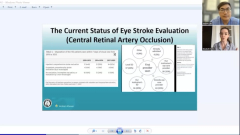
No, I've never found anything. So the issue is Claire Frazier says although most cases are idiopathic, there are some atomic and neurologic conditions that can mimic visual snow in the literature. And so the issue is, first of all, does that exist? And second of all, should we be doing an MRI and EEG and an ERG?
Elizabeth Fortin, MD:
Yes, so I think like we just discussed, what's really important is to take a very good history. And you have to know first what visual snow syndrome the idiopathic version looks like, and sounds like. So you have to make sure to take a good history and do a complete exam, including what we just mentioned, meaning you have to absolutely get a visual field and a macular OCT. She also suggests that you could get a fundus autofluorescence, which I haven't been doing regularly in my practice, but I think that could be a good idea if you have any doubts about the symptoms because you wonder if some patients that have a completely normal exam could have, for example, some retinal diseases that often that's sometimes present without any findings and fundus exam. So that is a good addition that you can think about doing if you're not completely certain that you have the idiopathic version of the visual snow syndrome. But otherwise, I think if you really do a good history and exam, you should be okay, without doing any further outside-of-the-office testing.
Andy Lee, MD:
Do you recommend they have an MRI?
Elizabeth Fortin, MD:
No, I normally don't recommend it myself. What about you?
Elizabeth Fortin, MD:
Most of the patients I see have already had an MRI. So it's very uncommon that I would see someone who hasn't had an MRI already. Probably a little bit different maybe in Canada, but I don't really recommend they have any testing. There have been some studies with fMRI and PET that showed the lingual gyrus is hyperactive I don't order any of those tests. Have you been ordering PET scans or fMRI or anything?
Elizabeth Fortin, MD:
Not at all because it doesn't change my management with these patients. So there's not really any treatments that has been convincingly shown to be working in these patients. So I don't do these routinely. I think it's more used for research purposes as of now. And maybe eventually we'll find a treatment that works for those those patients, but I personally haven't been doing them.
Andy Lee, MD:
I usually show the patients the other patients who have had fMRI and PET so that they know that I believe them. But I don't order a new one on them. How about EEG. Do you order that?
Elizabeth Fortin, MD:
So, EEG No. That's a good questions because we always wonder if there could be some patients who have for example, occipital seizures that could present with visual snow. But oftentimes, these people have other neurological symptoms, or their symptoms are intermittent, which can suggest that they have another condition such as migraine or seizures. So I don't routinely order EEG. What about you?
Andy Lee, MD:
I do not. Some patients with occipital seizure have little circles, but they're bigger and they're not like diffuse like the snow and they have like colored blobs in them. Unless there's some other evidence of seizure activity, I've not routinely been recommending EEG, electroencephalography. How about WRG? If you do ERG on those people?
Elizabeth Fortin, MD:
That's the same as same, pretty much the same answer. So if the exam is completely normal, again, including an OCT and a visual field, I don't normally do it. If you have a doubt also, one good way to approach these patients is to follow them in time. If you think that there is something that's not quite typical, you can see these people again, and if there's a change in their visual field or their appearance of the other retinal layer on the OCT, then you can probably think about doing an ERG. Now, again, there tends to be some finding either on the peripheral visual field and patients that have outer retinal diseases, or they can have findings on fundus exam. More specifically, if you don't have any fundus findings, if you do the fundus autofluorescence, as was suggested by Dr. Fraser, you're probably going to find something is if there's a patholody of the retina. So unless there's any of these I don't routinely order ERGs just also for a question of access, because it's not very easy, where I work to order to get an erg. What about you?
Andy Lee, MD:
I don't order any electrophysiology unless there's something on the exam that suggests it's retinol, about a word about treatment. Are you using any treatment on does anything work?
Elizabeth Fortin, MD:
I haven't been using treatments. So what I would say it's happened probably once or twice in people that were very, very anxious about the symptoms, and were about to change their career over the symptoms. Because of the symptoms. I haven't had any good success with them. There are medications that have been used such as Lamotrigine, sertraline, Topiramate, but I don't personally use them. What about you?
Andy Lee, MD:
We offer it to patients, mostly the anti anxiety agents help them with the coping mechanisms. And simple reassurance plus treating their underlying normal treatments for anxiety are helpful about Diamox? I've used Dynavox. What about Acetazolamide?
Elizabeth Fortin, MD:
So I haven't I mean, unless there are suggestions of increased intracranial pressure, I haven't I know there's no harm in doing it. But I haven't personally been using them.
Andy Lee, MD:
And what happens to these people? They just go away. They seem not to come back after a while in my practice.
Elizabeth Fortin, MD:
Yeah, they don't come back. After a while the symptoms don't tend to go away from my experience. I think they stay there. But, with reassurance, some people feel confident enough, and they know that they're not going to lose their vision. Oftentimes, I feel like reassurance is probably the most important part of what we're doing in the office. And, of course, you have to base your reassurance on a very complete and normal exam. And I think, oftentimes, this is enough to reassure them. I mean, maybe some end up going to my colleagues elsewhere, but I don't think so.
Andy Lee, MD:
I don't think so either, because I don't see a lot of second and third opinions on the snow. I think the first person is probably all they need. Well, maybe you could just give the take home message then from your perspective on should visual snow have any other testing?
Elizabeth Fortin, MD:
Yeah, so I think the take home is that you have to take a very thorough history on those patients and make sure you do have complete ophthalmic examination including a dilated fundus exam, you have to obtain an O CT of the macula and obtain a visual field testing. And if you have any doubt, there is no harm in obtaining an MRI and or an erg slash EEG depending on what the findings are. But, if you are confident enough and you have classic symptoms of idiopathic visual snow syndrome, it is okay, I believe, to do just the exam, the in-clinic ophthalmologic exam.
Elizabeth Fortin, MD:
I agree, Elizabeth. Well, that concludes yet another adventure with the NeuroOp Guru, and we'll see you guys next week. Thanks, again, Elizabeth. Goodbye.
Advertisement
Related Content
Advertisement




Latest CME






















Advertisement
Advertisement