
News|Videos|February 24, 2024
NeuroOp Guru: Venous sinus stenting for idiopathic intracranial hypertension
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Advertisement








Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss venous sinus stenting for Idiopathic Intracranial Hypertension
Video Transcript
Editor's note - This transcript has been edited for clarity.
Andy Lee, MD:
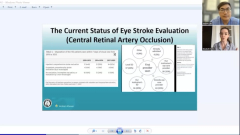
Hello and welcome to another edition of the NeuroOp Guru. I'm here with my good friend Drew Carey from Johns Hopkins. And today we're going to be talking about venous sinus stenting for Idiopathic Intracranial Hypertension in venous sinus stenosis. So Drew, maybe you could just give a little background on what the progress has been and how this paper helps us.
Drew Carey, MD:
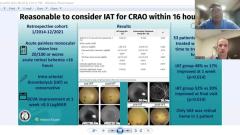
Yeah, so this is a review paper looking at various studies that have looked at outcomes of venous sinus stenting. As you know, most of us are familiar, Idiopathic Intracranial Hypertension is a vision threatening disease due to development of papilledema from elevated intracranial pressure and can cause progressive vision loss, and in 5% of patients can be blinding. And traditional treatments, things like weight loss for mild disease. Medications, like Acetazolamide to reduce intracranial pressure and the papilledema and protect vision. We have level one data for from the placebo controlled Idiopathic Intracranial Hypertension treatment trial. Surgical interventions, we don't have level one evidence for but in the past have included things like CSF shuntings, originally via lumbar shunts, and now more commonly via ventricular shunting. And optic nerve sheath fenestrations. Both of those are fairly invasive with the CSF shunting, having high failure rates and needing frequent revisions.
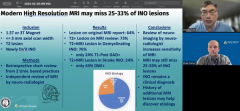
And we're not really sure how long optic nerve sheath fenestrations lasts for and there's a small risk of vision loss occurring with that procedure that we learned about from the Ischemic Optic Neuropathy Decompression trial. So maybe 2.5% risk of severe vision loss per surgery. For the last decade or two people have been looking at performing venous sinus stenting, as we have learned that stenosis between the transverse and sigmoid sinus is a very common feature of IIH. Present in probably 98% of more people. We're not sure if it's a chicken or the egg phenomenon.
Does it cause the elevated pressure? Is it a result of the elevated pressure? But it's become pretty apparent that it's at least a contributing factor. And that stenting these patients across the stenosis can result in a rapid and dramatic and essentially normalization of their intracranial pressure.
We don't have randomised controlled trials for this, either. So the authors have looked at collecting data from a number of these reports, because we know it lowers pressure. But what does it do for vision? What does it do for the patient's debilitating headaches? What does it do for the whooshing sounds in the ears that they frequently complain about? But as eye doctors we may not be prioritizing. What does it do for patients with double vision? And there's not been one great paper that looked at all of these, and many of the papers, looking at transverse sinus stenting really focused on pressure and haven't even looked at what happens to the papilledema and what happens to the vision.
So they said, hey, why don't we look at all the papers. And if we're going to plan a trial, this would be able to give us you know, some information for planning purposes like number needed to treat as well as information for counseling patients.
Andy Lee, MD:
So what about these symptoms? Did it work?
Drew Carey, MD:
Yeah, so you know, I think the most common symptom that patients experienced at least as reported by the IHTT was headache. And we saw a large number of headaches completely resolved, almost 50%. And an additional large number of patients had improvement in their headache perhaps ~20% of patients may have had persistent or maybe even worsening headache, which I think is what a lot of us have seen clinically, particularly in the first week or two. Patients may develop a new type of headache, as this metal foreign object is put in a blood vessel inside their head. For patients with pulsatile tinnitus, they saw about 82% of patients had resolution. Which is pretty dramatic because that doesn't usually resolve with shunting or with optic nerve sheath fenestration or with medication so that really may be getting at the primary etiology of this pulsatile tinnitus.
Patients with visual symptoms, which could include a variety of symptoms. The vast majority resolved at about 75% and the rest were unchanged. A very, very minimal amount of patients had worsening. Double vision for patients who had it at baseline, but prior to treatment, almost exclusively had resolution at greater than 90%. Transient visual obscurations also a huge amount of those patients resolved as well at about 80%. So I think that's pretty significant from the symptoms, right? Those are the things that patients really care about the things that are impacting their lives.
As far as you know, us being the eye doctors, the things that we really worry about, or prioritize is what happens to the papilledema and what happens to the visual field. And when they looked at outcomes from papilledema, putting all the studies together that looked at this, they had over 1000 patients, and about 40% of patients had total resolution of the papilledema, which is awesome. And another 43% of patients had improvement in papilledema. While very few patients, about 4%, were unchanged. Less than 0.5% of patients had worsening of papilledema, and about 4% of patients then developed optic atrophy. Those optic atrophy patients probably were going to be atrophic no matter what we did after the papilledema went away. So these are pretty promising.
Andy Lee, MD:
I think it's exciting. Even though we don't have head to head What is your sense about these efficacy numbers for symptoms and signs versus shunting? And for sheath fenestration?
Drew Carey, MD:
Yeah, I think you know, for sheath fenestration, we don't see a lot of patients getting resolution of headache, and certainly almost nobody gets resolution of pulsatile tinnitus. And double vision, also usually not something that's resolving for, you know, in the fenestration. Really when we're doing fenestration, we're trying to keep the patient from going blind tomorrow. It's not to control all aspects of the disease. I think we see a lot of patients improve in a number of these symptoms from shunting, although certainly not the pulsatile tinnitus and with shunting, some patients get new headaches, as well. You know, this paper, you know, they didn't highlight complication rates.
There's been other meta analyses, to look at complication rates and probably sit somewhere in between shunting and an optic nerve sheath fenestration. You know, if it was me, and I said, Well, you could put a shunt in your head or you could have two eye surgeries or you could get a stent, I'd probably up for stenting, knowing that, you know, you're gonna have to be on blood thinners to prevent instant thrombosis.
Andy Lee, MD:
How long do they have to be on the dual antiplatelet for? And what if they need a sheath fenestration afterwards or shunt?
Drew Carey, MD:
That's a great question. So our current practice is they're on dual anti platelet for 6 months. They do have studies where they have paused them to do lumbar punctures after a month or 3 months beforehand. And then the big question is long term, you know, nobody really knows what you need to be on after 6 months, as you know. Is baby aspirin once a day enough? Does it need to be you know, 2 or 3 times a week, or do you need anything?
That knowledge is still evolving. You know, they can be paused if you failed stenting and need to have a surgical intervention like a fenestration or a shunt. I know some folks will opt for fenestration first so you don't have to worry about that. And then stent later.
Andy Lee, MD:
That's kind of what we've been doing. If it's vision loss is the predominant problem and not the headache and the pulsatile tinnitus. We'll do the sheath fenestration. And then if we still have persistence of the headache, pulsatile tinnitus, not satisfied with the rate of recovery of the papilledema, it's stent versus shunt. And I think until we have a head to head, we probably are dealer's choice a little bit and it's gotta be individualized based on what the patient wants and how comfortable we are with the surgeon and the stent person.
Drew Carey, MD:
I agree. It's nice to have options and you know, it's takes a little bit more of a discussion with the patient. Sometimes they say just tell me what to do doc. And I say you tell me what to do. We'll talk about it. Does the patient's weight go into account at your institution for decision for stenting?
Andy Lee, MD:
Yeah, so it's much easier for our guys to consider the endovascular stent than the shunting procedure but maybe it's surgeon preference too based on weight. Same for you guys?
Drew Carey, MD:
Our neurology CSF center, who is mostly the gatekeeper for stenting has some evidence that folks with BMIs over 35 have higher rates of stent failure due to like adjacent restenosis and that might have improved as the stents have gotten longer. But they tend to prefer not to stent patients with a BMI over 35 in favor of other treatments if possible. I think some patients can still benefit absolutely from it. But they tried to get the BMI under 35. First, if possible.
Andy Lee, MD:
Neurosurgeons don't want to do shunt on obese patient either. So I guess maybe it doesn't matter. Nobody wants to operate on a morbidly obese person.
Drew Carey, MD:
Certainly not.
Andy Lee, MD:
What do you think the take home messages for this state of the art review? Is it still stay tuned? Or is it stenting works and is probably safe, and you should consider it on par with the consideration for the other procedures or in first-line?
Drew Carey, MD:
I think we would all certainly love to see a randomized control trial. It's going to be a challenge to organize that. I think at this point, the evidence is strong enough that it's certainly reasonable to consider if you need a surgical procedure on the same level as a fenestration or a shunt. Taking the patient's, you know, their individual preferences and risk tolerances. And if it's not happening in an institution near you, it probably will be soon so make friends with the interventional radiologist or a vascular neurosurgeon.
Andy Lee, MD:
I think that really is the bottom line. You got to use what you got. Certainly there are many places in Texas that don't have access to endovascular stent, but they can do a shunt and they don't even have sheath fenestration. So for a lot of Texas, it's pretty much shunt or you got to drive five hours,
Drew Carey, MD:
Go big or go home.
Andy Lee, MD:
Well, thank you, Dr. Kerry, as always for your expertise and input that concludes yet another edition of the NeuroOp Guru.
Advertisement
Related Content
Advertisement




Latest CME






















Advertisement
Advertisement