
Commentary|Podcasts|June 25, 2025
NeuroOp Guru: Using OCT to forecast outcomes in ethambutol optic neuropathy
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, discuss how baseline optical coherence tomography parameters can help ophthalmologists counsel patients and make more informed decisions after ethambutol-associated optic neuropathy.
Advertisement






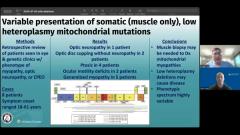


In this episode of NeuroOp Guru, host Andrew G. Lee, MD, discusses with Drew Carey, MD, how optical coherence tomography (OCT) may help predict visual outcomes in ethambutol optic neuropathy.1 Ethambutol, a cornerstone tuberculosis medication, can cause optic neuropathy with unpredictable visual prognosis.
Carey highlighted the need to stop ethambutol as soon as the diagnosis is made and acknowledged the challenge of counseling patients who often ask, “Am I going to go blind? Is my vision going to get better after I stop this medication?”
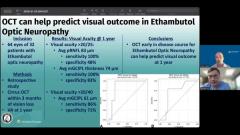
Carey reviewed a single-center, retrospective study of 64 eyes from 32 patients with ethambutol optic neuropathy. OCT scans were obtained within 3 months of visual loss, examining peripapillary retinal nerve fiber layer (RNFL) thickness and ganglion cell–inner plexiform layer (GCIPL) thickness as prognostic indicators at 1-year follow-up. “That has a 100% sensitivity for having a good visual outcome,” Carey explained, for patients with RNFL greater than or equal to 83 µm or GCIPL greater than or equal to 74 µm at baseline OCT.
These data can be especially useful in clinical practice. For patients presenting early with preserved RNFL and GCIPL measurements, practitioners can reassure them: “You can stop the medication now. We don’t have to worry about you losing vision down the line.” Conversely, in cases with lower thicknesses, providers can set realistic expectations for long-term visual recovery.
Although ethambutol-induced optic neuropathy is relatively rare in the United States, these findings support the utility of OCT in follow-up. Carey noted that “if you see a patient with clear ethambutol toxicity, OCT can help make sure that we’re going to get paid for using OCT for monitoring these types of patients.” However, he cautioned against using OCT for routine baseline screenings in all ethambutol patients: “I don’t think it’s been validated as a screening exam,” he said.
Carey noted that “it can help us predict who’s going to have a good vision at 1 year,” making OCT a valuable prognostic tool once ethambutol-associated visual impairment is evident.
Reference
Kang MC, Eun HW, Park KA, Oh SY. Optical coherence tomography parameters and optimal cut-off values for predicting visual prognosis in ethambutol-induced optic n neuropathy. J Neuroophthalmol. 2024;44(4):559-564. doi:10.1097/WNO.0000000000002092
Advertisement
Related Content
Advertisement



Latest CME


















Advertisement
Advertisement