
Commentary|Videos|April 2, 2025
NeuroOp Guru: Cranial nerve six palsy with chemosis is a critical clue to cavernous carotid fistula
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, return for this episode of 'NeuroOp Guru' to discuss how sixth nerve palsy with chemosis warrants suspicion for a cavernous carotid fistula, emphasizing careful examination for dilated conjunctival vessels and the need for imaging for accurate diagnosis and timely intervention.
Advertisement






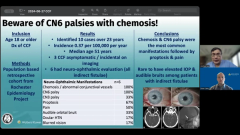


This latest episode of the “NeuroOp Guru”—hosted by Andrew G. Lee, MD, from Houston Methodist, and joined by Drew Carey, MD, from Johns Hopkins University—features the importance of recognizing cranial nerve six (CN VI) palsy with chemosis as a potential sign of a cavernous carotid fistula (CCF). This condition, particularly the low-flow type, can be challenging to diagnose due to its rarity and overlapping features with more common conditions like thyroid eye disease.
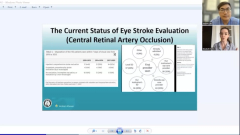
The discussion centered on a population-based study1 from the Mayo Clinic using data from Olmsted County. The study identified only 10 cases of CCF over 23 years, emphasizing its low incidence of 0.37 per 100,000 patient-years. The median age at diagnosis was 51. All patients with neuro-ophthalmic evaluation exhibited chemosis and CN VI palsy, with other common findings including proptosis, third nerve palsy, and audible bruits. Notably, only half of the patients reported pain, potentially contributing to delayed diagnosis.
The key clinical takeaway is that CN VI palsy with a red eye should not be mistaken for a microvascular palsy. Careful examination of conjunctival vessels is crucial—dilated, corkscrew vessels extending to the limbus suggest elevated venous pressure and a likely fistula rather than thyroid eye disease.
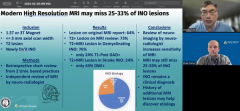
Regarding imaging, noninvasive modalities like CT or MRI can suggest CCF by detecting a dilated superior ophthalmic vein. However, CTA and MRA have limitations, especially in low-flow fistulas, due to challenges in visualizing contrast drainage. A conventional catheter angiogram remains the gold standard for definitive diagnosis.
Ophthalmologists should maintain a high index of suspicion for CCF in patients with CN VI palsy and chemosis, as early detection and appropriate imaging are crucial for timely intervention.
Reference
Cohen DA, Sanchez Moreno FR, Bhatti MT, Lanzino G, Chen JJ. Evaluating the incidence and neuro-ophthalmic manifestations of carotid-cavernous fistulas. J Neuroophthalmol. 2024;44(2):232-235. doi:10.1097/WNO.0000000000001973
Advertisement
Related Content
Advertisement



Latest CME


















Advertisement
Advertisement