
Blog|Videos|June 5, 2024
NeuroOp Guru: High-resolution MRI may miss a third of INO lesions
Author(s)Andrew Carey, MD, Andrew G. Lee, MD
Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss how modern high-resolution MRIs may miss up to a third of internuclear ophthalmoplegia (INO) lesions
Advertisement








Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss how modern high-resolution MRIs may miss up to a third of internuclear ophthalmoplegia (INO) lesions
Video Transcript
Editor's note - This transcript has been edited for clarity.
Andy Lee, MD:
Hello, and welcome to another edition of the NeuroOp Guru. I'm here with Dr. Drew Carey from Johns Hopkins.
Drew Carey, MD:
Hey Andy.
Andy Lee, MD:
And today we're going to be talking about how even modern high-resolution MRI could miss up to a third of internuclear ophthalmoplegia lesions. And so Drew, maybe you can just tell us what an INO is, and what would that look like clinically?
Drew Carey, MD:
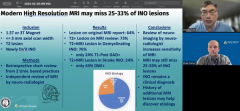
Absolutely. So an internuclear ophthalmoplegia is caused by a lesion in the medial longitudinal fasciculus, which connects the sixth nerve nucleus and contralateral third nerve sub-nucleus of the medial rectus. And this is an important structure because it helps helps maintain lateral gaze. So if you're looking to the left, you need your left eye sixth nerve to innervate your lateral rectus and your right third nerve to innervate the medial rectus. And they have to do it in a coordinated manner. So both eyes move at the same time as opposed to one eye and then the other eye, and then you get double vision. If you have a lesion there, oftentimes you see the one eye has an abduction deficit so it doesn't look well towards the nose and the other eye moves pretty well except it has a AB ducting nystagmus, and it's very classic appearance. It's not a third nerve palsy. It can be associated with other findings like skew deviation. But there's it's very well localizing and depending on your age group has very typical causes that we may need to identify because of other neurologic implications of this disease processes.
Andy Lee, MD:
So by age group, you mean if you're young, you have demyelinating lesion. And if you're old, you have an ischemic lesion.
Drew Carey, MD:
Yes, that is what I mean. And it's different from our ischemic cranial nerve palsy is because this is in the brainstem. So it's a parenchymal ischemia, which means it's a stroke. And while patients may improve with time, if you have a stroke, you're at risk of having further strokes. And so they need stroke modification, and assessments to decrease the risk of having further strokes.
Andy Lee, MD:
And so what were the results of this study with MRI with INO?
Drew Carey, MD:
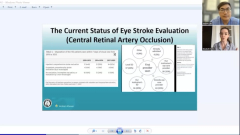
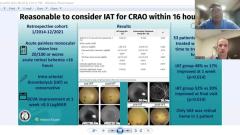
So they looked at this the single institution, and they looked at patients who had an INO, and they had to have an MRI imaging on a 1.5 Tesla or three Tesla magnet. So these are modern, fairly high resolutions. They had to have good quality scans less than or equal to three millimeter axial slices. And they were looking for T2 lesion and a newly diagnosed INO patient and so. Done at two different universities. They had an independent review of of all of these MRIs by a neuroradiologist. They looked at the original reports, and they said that only 64% of them on the original report, were able to identify the lesion. When they reviewed them, they did see a T2 hyperintense lesion on 73% of those MRI scans. And in patients with demyelinating disease, they were able to find a lesion of T2 hyperintensity in 76%. But only 24% of them were enhancing, which is a separate but interesting point. And then in the stroke patients, the T2 hyperintense MRI lesions, were present in 24%. And they only had diffusion weighted imaging changes in 43%. So, you know easy to find in MS, harder to find in a stroke.
Andy Lee, MD:
Is DWI supposed to be for stroke, shouldn't you see restricted diffusion or it's too small?
Drew Carey, MD:
You know, a lot of times these lesions are really small. And I think that's the problem and it may not be quite as good in the brainstem because when you get to tissue interfaces, there's a lot of distortion like it's really hard to see that in an ischemic optic nerve injury. And you have–it's a small area and surrounded by cerebral spinal fluid and then you have the aqueduct there so you can get a lot of artifacts.
Andy Lee, MD:
Shouldn't the demyelinating lesion that's acute be enhancing, or same problem?
Drew Carey, MD:
I think it's the same problem, you know, we'd like to think that the slices are perfectly correlated on your T2 and on your T1 post contrast, but they might not be perfect and so you may miss it.
Andy Lee, MD:
Do you admit the INO if it's a stroke, demyelinating, either, both?
Drew Carey, MD:
You know, I call on my neurology colleagues. I think most of them do get admitted for rapid stroke workup to see what risk factors they have and what we can do to minimize them. Now, granted if it's a small lesion, most of the time right, this is hypertensive injury, and small vessel disease. But that doesn't mean they can't also have atrial fibrillation, carotid stenosis, [inaudible] dissection, embolic disease from cardioembolic etiologies, and so those do need to be evaluated. For the demyelinating patients, you know, depends on how disabled they are. If they have known demyelinating disease, we definitely need to coordinate with their neurologist to say; Hey, they're having active brainstem complications, and that has a really poor long term prognostic factor. If they're really disabled by it, then we know that mega dose, or postdose IV steroids do help to speed recovery. If it's minimal, and they have known disease, they may not need to, if it's a new person, and that's their presenting symptom, then usually they're gonna end up being admitted. Absolutely.
Andy Lee, MD:
So what do you think the take home message for our audience is from this study?
Drew Carey, MD:
I think the major take home point is the clinical exam is really crucial in these patients, because it's going to tell you where the lesion is, and tell you that it's a brainstem parenchymal lesion. And that just because you don't see it on the MRI doesn't mean it's not real and the patient doesn't have a real disease, and that does not have serious neurologic complications if it's not diagnosed and treated appropriately. So I think all our general ophthalmologists and neuro ophthalmologists need to, you know, remember that the exam is important and coordinate with our neurology colleagues for the appropriate care of these patients.
Andy Lee, MD:
And I think we always tell our residents, we treat patients, not those MRI scans. The MRI just confirms what we already think. And if you think it's an INO, we're going to treat it as an INO, and work it up as an INO.
Drew Carey, MD:
Yeah. And that MRI can tell us other things like is it multiple sclerosis, or do they have other silent strokes occurring that you know, tell you multiple vascular distributions, think about cardioembolic disease, but that specific lesions is a clinical diagnosis. Absolutely.
Andy Lee, MD:
Well, that concludes another edition of NeuroOp Guru. Thanks again, Dr. Carey.
Drew Carey, MD:
Thank you for having me. Dr. Lee.
Advertisement
Related Content
Advertisement




Latest CME



















Advertisement
Advertisement