
Commentary|Podcasts|June 2, 2026
NeuroOp Guru: Stopping GLP-1 therapy may trigger recurrent papilledema in IIH cases
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, discuss recurrence of papilledema after discontinuation of GLP-1 receptor agonists and the implications for monitoring patients with idiopathic intracranial hypertension.
Advertisement








In this episode of
Lee is the chair of the Blanton Eye Institute at Houston Methodist Hospital and a professor of ophthalmology, neurology, and neurosurgery at the Weill Cornell Medical College. Carey is the Neil R. Miller Rising Professor of Ophthalmology in the division of neuro-ophthalmology with the
Carey reviewed the growing evidence supporting GLP-1 receptor agonists in IIH, noting that these
Stopping GLP-1 therapy may increase the risk of recurrent papilledema
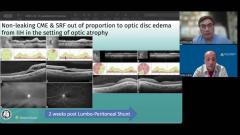
The discussion centered on a 31-year-old woman with longstanding severe IIH and prior optic nerve sheath fenestration who developed recurrent headaches, pulsatile tinnitus, and worsening papilledema approximately 1 month after discontinuing semaglutide.1 Although visual field loss remained stable in one eye, progression of central and nasal scotomas in the fellow eye raised concern for worsening vision loss related to recurrent papilledema.
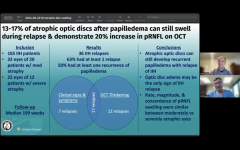
Carey emphasized that recurrence after stopping GLP-1 therapy remains a newly recognized phenomenon, and clinicians currently lack standardized monitoring protocols for patients discontinuing these medications. Although not all patients experience recurrence after treatment cessation, individuals with advanced baseline vision loss or optic disc pallor may be particularly vulnerable to further visual decline.
The conversation also highlighted the importance of counseling patients about symptom recurrence after medication discontinuation, including worsening headaches and pulsatile tinnitus, which may signal rising ICP. Carey suggested that closer follow-up after stopping GLP-1 therapy—particularly within the first 1 to 2 months—may help identify recurrent papilledema before significant visual deterioration occurs.
The discussion reinforces the emerging role of GLP-1 receptor agonists in IIH management while underscoring the need for structured monitoring strategies when these medications are discontinued, especially in patients at high risk for vision loss.
Reference
Phillips MJ, Gokoffski KK. Recurrent idiopathic intracranial hypertension-related papilledema after abrupt discontinuation of semaglutide. J Neuroophthalmol. 2025;45(4):e283-e284. doi:10.1097/WNO.0000000000002293
Advertisement
Related Content
Advertisement





Latest CME



















Advertisement
Advertisement