
Commentary|Podcasts|February 5, 2026
NeuroOp Guru: Understanding optic disc cupping after optic neuritis
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, discuss how optic disc cupping after optic neuritis reflects nerve and ganglion cell thinning, not disease type, helping distinguish it from glaucoma.
Advertisement








In this episode of
Lee is the chair of the Blanton Eye Institute at Houston Methodist Hospital and a professor of ophthalmology, neurology, and neurosurgery at the Weill Cornell Medical College. Carey is the Neil R. Miller Rising Professor of Ophthalmology in the division of neuro-ophthalmology with the
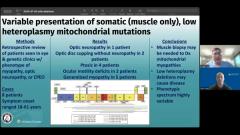
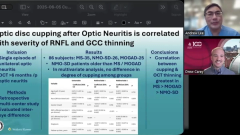
Carey introduced the study: “This was a multicentered retrospective study looking at patients who had a single episode of unilateral optic neuritis, and they looked at their optical coherence tomography that had to be a minimum of 6 months after onset of their optic neuritis.” The study included 35 patients with multiple sclerosis-related optic neuritis, 26 with neuromyelitis optica spectrum disorder, and 25 with myelin oligodendrocyte glycoprotein antibody–associated disease.
The purpose of the study was to determine whether post-optic neuritis cupping is disease-specific, age-related, or correlated with structural damage to the optic nerve. Carey noted, “Some of these nerves are really cupped, and maybe they get misdiagnosed as glaucoma. Is this a disease-specific finding, or is this related to the severity of their vision loss, or what's the reason they get this cupping?”
Cupping correlates with structural damage, not disease type
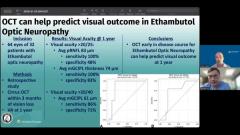
The study found no difference in cupping among the 3 groups and no correlation with age or gender. Instead, cupping correlated with the severity of RNFL and ganglion cell complex thinning. Carey emphasized, “We're not talking about huge degrees of cupping in these patients. On average, it was about .07 cup-disc ratio difference between the two eyes, with some eyes going up as high as maybe .2 in severe cases.” He explained that more structural damage predicted more cupping, establishing it as a correlate of optic neuropathy severity rather than disease type.
The discussion also addressed clinical implications. Carey advised, “You don't have to be concerned that there's a .1 or .2 difference between these 2 eyes in this patient who had optic neuritis. That cupping is not glaucoma… We're seeing cupping typically in these patients, and the more thinning there is, the more cupping.” He noted that glaucoma evaluation may still be appropriate if the cup-disc ratio difference is disproportionately large relative to RNFL thinning. Carey added, “If I'm concerned that the patient has glaucoma in addition… that patient I might send to the glaucoma specialist… But I think that's pretty rare.”
Carey concluded with practical guidance: when optic neuritis patients have cupping, clinicians should recognize it as a potential sequela of structural optic nerve damage rather than immediately attributing it to glaucoma. Communication with glaucoma specialists is essential if coexisting glaucoma is suspected, as it informs intraocular pressure targets and management decisions.
The conversation reinforces that optic disc cupping after optic neuritis is a structural correlate of nerve fiber loss rather than a disease-specific marker or sign of glaucoma.
Reference
Estrela T, Stiebel-Kalish H, Rettenmaier L, et al. Optic disc cupping in neuromyelitis optica spectrum disorder, myelin oligodendrocyte glycoprotein antibody-associated disease, and multiple sclerosis and its relationship with optical coherence tomography parameters: a multicenter study. J Neuroophthalmol. 2025;45(2):164-169. doi:10.1097/WNO.0000000000002204
Advertisement
Related Content
Advertisement




Latest CME




















Advertisement
Advertisement