
News|Videos|February 17, 2024
NeuroOp Guru: Benefits of mindfulness-based cognitive therapy for visual snow syndrome
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Advertisement








Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss a study showing the benefits mindfulness-based cognitive therapy for Visual Snow Syndrome.
Video Transcript
Editor's note - This transcript has been edited for clarity.
Andy Lee, MD:
Hello, and welcome to another edition of the NeuroOp Guru. I'm here with my good friend, Drew Carey. Hi, Drew.
Drew Carey, MD:
Hi, Andy.
Andy Lee, MD:
And today we're going to be talking about the open label feasibility study demonstrating benefit of mindfulness based cognitive therapy customized for the visual snow syndrome. So Drew, maybe you could just tell us on a little bit about visual snow and what they tried to do in this study.
Drew Carey, MD:
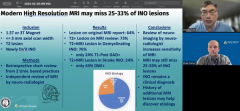
Absolutely. So Visual snow is this condition that we're only just beginning to learn about. We don't have a great understanding of what it is or what causes it. And a lot of the research has actually been patient driven by groups of patients getting together and helping to inform their doctors and which has been really amazing and helpful. But one of the common or unifying features is patients see, what sometimes they'll refer to as snow or static, similar to what's on the old fashioned TVs when they didn't have a signal coming in. Where it's either black or white dots in the visual field, all throughout the visual field. So non localizable. They tend to move, they may have a little bit of flickering in them. For some patients, they're more visible on light backgrounds, like a computer screen, or bright blue sky. Some patients will see them actually more in dim lighting. And they are for the most part present all the time. Most patients will probably tell you they've had it their whole life, and they thought that's just what normal vision was like. And we've not been able to really find an identifiable lesion on MRI in these patients. Sometimes there are some mild changes in the hypothalamus when compared to healthy controls. And so we think there may be a wiring or filtering abnormality in the visual processing system that allows their brains to see this stuff that maybe is all there and the rest of us are filtering it out. And then there's been some functional MRI studies showing actual increased connectedness between various visual processing centers in the brain, also suggesting that there's this filtering problem or hyper perception.
Andy Lee, MD:
So what did they try to do with this mindfulness, cognitive therapy?
Drew Carey, MD:
Yeah, so we've been very limited in our ability to to help these patients with medications with some of our, you know, favorite toolkits of antidepressants or anti epileptics that we may use for patients with migraines or persistent visual auras. And so these folks said, hey, let's let's stop trying to throw medicines at them. And instead, why don't we work on mindfulness based cognitive therapy. In which they teach some kind of coping skills, when they're seeing the visual symptoms, when they're being bothered by them, you know, ways to kind of distract themselves, you know, to be aware of their symptoms. And then to kind of focus awareness somewhere else. And so these are a common psychotherapy skill that's used for a lot of other disorders that we don't have medicine for, that patients find significant benefits from by reducing psychologic features that are brought on by unpleasant thoughts or feelings or body sensations. And this is really targeted for the visual symptoms. And so they it was an 8 week, open label study in which they would have therapy sessions and be taught these skills. And they had them evaluated at baseline at week 9, so when they finished the therapy, and then week 20, and they could continue to practice these skills at home, but they wanted to see did they lose the effect? Or did they have persistent benefit without having to partake in intensive therapy studies.
Andy Lee, MD:
They have radiographic correlate too?
Drew Carey, MD:
They do. They did functional MRI, to see if there was any benefit that was noticeable there. Which I think is a really cool thing to do. It couples, kind of what we as clinician scientists, you know, think of is as the hard data with what the patients really care about, right? The patient reported outcomes, how's their anxiety, how's their quality of life? And I thought that was a really clever evaluation, or way to design this study.
And how much does it cost, do you think? Or they didn't say?
I don't know how much it costs. I think it depends on the healthcare setting that you're in. This study was undertaken in the In the UK, I believe and so they have a much different health care system than we do in the United States. Certainly MRIs cost, and functional MRIs have a cost associated with them. Certainly you don't need to have that if you're going to undergo therapy, that was certainly part of the research protocol to add strength to their findings.
Andy Lee, MD:
So have you tried this on anybody?
Drew Carey, MD:
So I'm not a licensed psychotherapist. I have had some visual snow patients come to see me in whom I've discussed the results and that they may benefit from partaking in a mindfulness based cognitive therapy for visual symptoms. I haven't had anybody come back to tell me how they've done with it. But I think a lot of patients, like the idea, you know, they know it's something they've had for a long time, they're not crazy about taking medication for it, you know, especially medications, the these types of medications can have significant side effects. And they've had it their whole life, which means they'd have to, even if there was a benefit from medication, they'd have to take it for the rest of their life. And most of them are not that excited about it. You know, in the past, usually reassurance you told them good news is you're not going blind. There's never been anybody who's gone blind from this, you know, is what most patients have kind of looked for in the past. But for those who are significantly bothered by it and worry that it impacts their quality of life, and it's anxiety provoking. I think this is a really, you know, really good option for them. And as we learn more, maybe we'll get more options. But for now, this is the best result we've had from from anything that's been tried.
Andy Lee, MD:
Well, I've certainly thought about recommending it more. Like you, I don't do it myself. But we do know people who do it for other things, as you mentioned, and it certainly helps those patients as well. So I'm willing to give it a try. So stay tuned to this channel, I think is the take home message.
Drew Carey, MD:
Absolutely.
Andy Lee, MD:
And Drew, it's very good to see you again. Thank you so much. That concludes another edition of NeuroOp Guru.
Advertisement
Related Content
Advertisement



Latest CME


















Advertisement
Advertisement