
|Videos|January 6, 2023
NeuroOp Guru: Thymectomy in ocular myasthenia gravis, yes or no?
Author(s)Andrew G. Lee, MD, Elizabeth Fortin, MD
On this week's episode of the NeuroOp Guru video blog, Andy Lee, MD, and Elizabeth Fortin, MD, discuss Thymectomy in Ocular Myasthenia Gravis, Yes or No?
Advertisement








Andy Lee, MD: Hello, and welcome again to another edition of the NeuroOp Guru. I'm here with my good friend, Elizabeth Fortin. Hi, Elizabeth.
Elizabeth Fortin, MD: Hi.
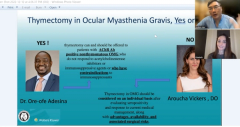
Lee: And today's topic is Thymectomy in Ocular Myasthenia Gravis, Yes or No? and it follows what was already published by our colleagues Dr. Ore-ofe Adesina and Aroucha Vickers, Do, and so maybe you could just articulate for the audience, what would the pro and con positions are, and then we can chat about what we really should be doing.
Fortin: Of course, So I think the proposition stems a lot from the literature mostly on the generalized myasthenia gravis. So there's been a lot more information on people with generalized myasthenia gravis over the past years. We've known for a long time that patients with thymomas of course need thymectomy for obvious reasons. It's in patients with non-thymomatous myasthenia gravis that we wonder if they can benefit from thymectomy. People with positive antibodies which most people with generalized myasthenia gravis have positive antibodies seem to benefit in the long term from thymectomy. And there's more and more evidence towards that. But the evidence is not as clear for ocular myasthenia gravis. And so in the pro, I think one of the consideration would be, is there a chance that we can reduce the rate of generalizations in our patient with ocular myasthenia gravis? And is there a chance we can improve their outcome as well. There's been a couple of studies on this, but the evidence is not very strong. And I think that leads me to speak to the cons portion of this, which Dr. Vickers discussed. Every time you consider doing a surgery on a patient, you have to consider all the risks associated with the procedure. More and more the time activities are done with the non-invasive methods. So I think we're seeing a reduction and risks associated with the procedure, but it's still a surgery. We have to consider the risks and the benefits for patients. And I think also in the cons, well, of course, so you have the surgical risk associated with it. You also have, you know, to make the diagnosis in a timely manner. So in order to prevent generalizations, you have to make sure that you diagnose these patients early enough to prevent generalization and often that we know that ocular Myasthenia is often diagnosed late because of the various presentations that can be confused with other conditions. I think that sums the bigger points. I don't know if you had something to add Andy on this.
Lee: So are you saying that if they have a thymoma they have to have surgery, no matter whether it's ocular or general?
Fortin: Yeah, exactly.
Lee: This is non-thymomatous. How do they know whether it’s thymic hyperplasia or thymoma? How can they even tell that by looking at a scan? Or do you think they can tell that?
Fortin: I think I think most of the time, they're able to tease those apart now with the most precise imaging modalities that we have. But sometimes there's definitely a gray zone of overlap between the two where I think it's difficult to tease those apart. Patients who have positive antibodies most commonly will have some type of anomalies of their times, right. Whether 60 to 70% will be hyperplasia, but then there's a 10 to 12% that would be thymoma. And I think in those patients with thymic anomalies, it's an even better question, even in our patients with ocular myasthenia as to whether they could benefit from thymectomy.I think that's where we, we kind of wonder if some of these patients could go could benefit from the intervention even in the ocular population.
Lee: And do you agree that they have to fail medical therapy or have a contraindication to immunosuppression before you would consider thymectomy? Or do you think you can do it even without those parameters?
Fortin: I think, in 2022, we still consider immunotherapy, or you know, medical therapy as the first line. And the consensus that were updated in 2020 also agree with that statement. So it seems like the first line of treatment remains medical therapy. We know that most of our patients have a very reasonable profile of side effects with the medicine because it's either acetylcholine esterase inhibitors, which are which are well tolerated, or low dose steroids plus or minus, you know, other immunosuppressants. But they normally tolerate the medicine pretty well. So I think it's true to say if we consider the risks of the surgery, that we should reserve that for patients with, you know, who fail medical therapy. But I do think that this may change in the future there is, you know, significant evidence that we can prevent generalization in our patients because again, we have to remember there's almost 50% of our patients end up having generalized disease. Is that your opinion as well?
Lee: Yeah, that's been my experience as well. And do you use neurology for all these cases? I don't personally think ophthalmology should be trying to determine whether someone's generalized or not They need a neurologist.
Fortin: I agree. I think they need a neurology assessment. And this is a good example of where co-management is the best, in my opinion, option for patients.
Lee: So what would be your take home message on thymectomy and ocular myasthenia gravis?
Fortin: I think it's reasonable to consider thymectomy in non-thymomatous antibody positive ocular myasthenia gravis, when they fail medical therapy. But we should still keep medical therapy as a first line treatment, as of now.
Lee: But everybody has to have imaging of their chest, and it can't be a chest X ray.
Fortin: Everybody. CT.
Lee: I think we are in agreement once again, Elizabeth. And I thank you for your time. And we'll see you next time on the neurotic guru.
Fortin: Thank you
Advertisement
Related Content





Latest CME






















Advertisement
Advertisement