Now Playing

On this week's episode of the NeuroOp Guru video blog, Andy Lee, MD, and Elizabeth Fortin, MD, discuss the comparison of the range of lumbar CSF pressure in adults with normal CSF pressure and in idiopathic intracranial hypertension.
Andy Lee, MD: Hello, and welcome to yet another edition of the NeuroOp Guru. I'm here with my good friend Elizabeth Fortin.
Elizabeth Fortin, MD: Hi.
Andy Lee, MD: And today, we're going to be talking about the comparison of the range of lumbar CSF pressure measurements in adults, both with normal CSF pressure and an Idiopathic Intracranial Hypertension. So Elizabeth, maybe you could just set the stage for us and tell us why do we even need to know this?
Elizabeth Fortin, MD: Yeah, so there's been a lot of change in our understanding of what the normal CSF pressure is. We used to use a much lower upper limit for the CSF pressure, which was set at 20 at some point. We realized that probably some normal individuals have higher ICPs than 20. So the with more studies, we raised that upper limit to 25, and that's what we use currently in our guidelines to diagnose IIH. And it's important for us, especially in neuro ophthalmology, because when we diagnose Idiopathic Intracranial Hypertension, the ICP raises one of our criteria on top of other things, as you know, like optic nerve head swelling and other symptoms. We use this as one of our diagnostic criteria, so that's why it matters for us to know, what is the actual normal range and in patients who don't have IIH.
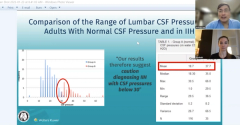
Andy Lee, MD: And so this table here, Table 1, has Group A normal and Group B. And I see you have put a red box around the mean. Maybe you could just walk us through these numbers and tell me what you think these mean to us as physicians.
Elizabeth Fortin, MD: I think what's interesting in that table is, first of all, of course, the mean, gives you an idea of what normally our patients with normal CSF pressure, what their CSF pressure is around, so 18.7 for them. And group B is the IIH population where it's much higher. So the mean was 37.7. The other interesting part, if you go lower, is the range. The range in the normal CSF pressure group was 1 to 29.5. And then the group with increased intracranial pressure was 29 to, I think it was to 66. So there is a small overlap. And I think we can look at the bar chart on the left hand side. And that's also useful because it's very visual. So you see that there is an overlap between the normal ICP population and our population of patients with Iron Age, but the overlap is quite small as at least in that study. So in this study, there was only one patient in the normal ICP group that had a ICP higher than 29. And that was one value of 30.5. And there was also only one patient in the IIH population that had it a pressure of below 30. So that was interesting to me to see how little the overlap was between the two groups. And I think one strength of that study is that the lumbar punctures were performed by only one operator. So the same skilled operator was performing all the LPs. And I really think that that can have an impact on the reliability of the results.
Andy Lee, MD: And so the little quote, here is our results therefore suggest caution, diagnosing IIH with CSF pressures below 30. Do you think that is the correct conclusion from these results?
Elizabeth Fortin, MD: I think, to me, my understanding of that study is that, you know, sometimes we have patients in whom we do we perform a lumbar puncture. And the diagnosis says is not obvious based on just the appearance of the optic nerves and the symptoms and the findings on MRI. And then if we have a pressure between 25 and 30, then we might want to use caution with the diagnosis and just think that this could be a normal ICP. Before, we used to think that over 20 was an abnormal or elevated ICP, and we know that this has been constantly evolving over time. So I think it's to be cautious with the ICP, and that the normal might be higher than what we previously thought. I don't know what your interpretation of this would be.
Andy Lee, MD: Well, I kind of view it like IOP. So ICP and IOP. but like glaucoma of the eye but like glaucoma of the brain. And so in glaucoma of the eye, we learn that 20 number also, but 20 millimeters of mercury for the IOP like 20 centimeters in water for ICP. And what we learned I think from glaucoma is there are people that have normal tension glaucoma, but they're also people that have high pressure that are ocular hypertensive, but they're not glaucoma, they're just glaucoma suspects. And I suspect that's the same thing here, where there is two overlapping curves. Normal people who have high pressure but nothing's wrong with them, and people who actually have papilla edema, but their pressure is borderline, or they have clearly IIH and their pressure is borderline. So to me, it's not so much the number as it is being cautious anytime we're within one standard deviation of the mean. And so to me, what this paper means is, if you get a number of let's just say the mean was 18.7, and you add a standard deviation of 5.2. And you're talking about to beware of numbers in the 23 to 25 range, because that's only one standard deviation from the mean. And that means you could be normal people or one standard deviation and the mean, but there's nothing wrong with them. And I think the same thing applies the other way, which is 37 was their mean, but their median was 35, and a standard deviation of 8. So, if you take 35 and you take away 8, you're talking about 27 or 28, something like that. And so that means some of those people with 27s still have it. So, for me, it's not about the number 30, which they chose. I think we're still in the same ballpark of what we use. We are used to 20 to 25 being borderline. And by borderline, what you mean is one standard deviation from the mean. Twenty-five and above is like an IOP of 26. You're like, Okay, this is probably glaucoma, but there's some people who are two standard deviations from the mean, and they still don't have glaucoma. And so I think this helps add up to make the number that we'll accept, higher rather than lower. I don't think it changes what I do in terms of practical if the person looks like papilledema. I'm still going to treat that even if the pressure is borderline. But it is useful to have some numbers and I think it's a quite fascinating thing, as you mentioned, and that the line seems to divide it at 25 to 30. Somewhere in there is where the red and the blue in the left hand panel are seeming to overlap. And that means we're going to over diagnose some people, but we would underdiagnose some people if we put the number 30 there.
Elizabeth Fortin, MD: Exactly. And we have to remember that in real life and our LPs are going to be performed by different people. And sometimes you can lose some fluid when you put the manometer on and so, you know the perfect technique is not doesn't, you know, really apply to real life. So I think I completely agree that with like with any diagnosis, we have to use our clinical judgment. And now we just know that maybe you know, the higher limit of normal might be a little more than what we thought but I don't think it's going to change my practice either.
Yeah, so I always tell the residents treat the patient, not the number. And we treat people not pressures. But it is a fascinating thing, and I thank you for your time again, Dr. Fortin. And this concludes yet another edition of the NeuroOp Guru. We'll see you again next week.
Elizabeth Fortin, MD: Yes, thank you.






















