
News|Videos|April 13, 2024
NeuroOp Guru: Susac syndrome and fluorescein angiogram
Author(s)Andrew Carey, MD, Andrew G. Lee, MD
Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss Susac syndrome, and how leakage on fluorescein angiogram might be the most sensitive marker of activity of disease.
Advertisement








Andrew Lee, MD, and Andrew Carey, MD, sit down on another episode of the NeuroOp Guru to discuss Susac syndrome, and how leakage on fluorescein angiogram might be the most sensitive marker of activity of disease.
Video Transcript
Editor's note - This transcript has been edited for clarity.
Andy Lee, MD:
Hello and welcome to another edition of the NeuroOp Guru. I'm here with my good friend Dr. Drew Carey from Johns Hopkins. Hi drew.
Drew Carey, MD:
Hi, Andy.
Andy Lee, MD:
And today we're going to be talking about a very unusual condition – Susac syndrome. And how leakage on fluorescein angiogram might be the most sensitive marker of activity of disease. And so maybe Dr. Carey, you could just fill us in on what exactly is Susac, and how would it present and why do we need this angiogram.
Drew Carey, MD:
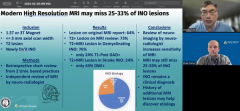
Susac Syndrome is a rare vasculitis. It has a triad of symptoms, but most patients probably don't meet all three characteristics. The one as ophthalmologists and neuro-ophthalmologist that we're most familiar with, is multiple branch retinal artery occlusions, not due to an embolic phenomenon. And these can happen sequentially, and in rapid progression, and patients can have really severe visual field loss from that. And neurologic manifestations, most commonly [include] dizziness and imbalance but they can also have confusion. And they can have very characteristic MRI findings. Their corpus callosum is that particular risk of injury in this condition. And they can, it can have a Swiss cheese like appearance. Sometimes patients show up with an encephalitis like picture and they see the findings on MRI scan and they say well, let's get an ophthalmology consult. Sometimes they present to like an E&T doctor for dizziness or hearing loss.
Andy Lee, MD:
And so just walk us through maybe the imaging, the audiograms here and then we'll end with the angiogram, which is I think the point of the paper. But in terms of the infographic just for completeness sake.
Drew Carey, MD:
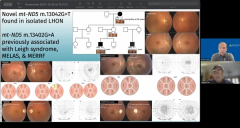
Absolutely. And I am not an ear, nose, and throat or hearing specialist, so the audiograms are not my area of expertise. But patients often present with hearing loss and they can test them at different frequencies. And in these Susacs patients can have hearing impairment, I believe it's it's more so at high frequency type of hearing loss. Different than what you would expect in patients who are in jobs that would put them at risk for hearing loss due to loud sounds like musicians and people working in the military. And so that is a big concern. In the MRI scans that we see in the bottom left and bottom right, we see kind of these small vessel pericallosal, white matter changes that we can see sometimes in age-related manifestations, but even in a young person, you would not expect to see that. Although maybe you would see it in migraine patients or those with seizures, but absent that kind of history, you would not expect to see that. In the bottom right hand we have the T1 sagittal midline showing the corpus callosum and we see this hypo-intense lesion right in the middle of the corpus callosum. That's, one of these corpus collosal lesions. And if you get a lot of them that leads to Swiss cheese kind of appearance there and in the chronic phase, you just get an irregular thinning of the corpus callosum. And, sometimes that's a clue to, you know, patients who have more of a smoldering or chronic disease when they come in.
Andy Lee, MD:
And so how about these angiograms? What was the point of the paper?
Drew Carey, MD:
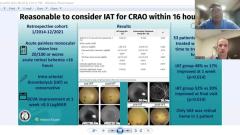
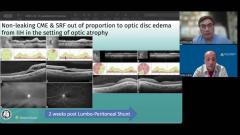
One of the challenges, you know, now that doctors have gotten better at diagnosing Susacs, and especially if the patient comes in acutely with the triad of symptoms, we say, okay, we know what this is, we're going to put you on the immunosuppression that we think works best for this. Whether it's something like mycophenolate or IVIG or plasmapheresis. But then the challenge after you've learned how to diagnosis and treat the acute stage is maintenance therapy and monitoring. So how do we know that patient is in remission? Or do they have disease recurrence? And do we need to escalate or maybe is it safe to taper because they've been quiet for a number of years. So what they really wanted to do was look at patients who have had are in the chronic stage and see if we can help to distinguish who's active or inactive – who's at risk of further vision loss. And so what they found in the paper and some of these fluorescein angiograms show is that staining of an arterial, particularly at a non-branch point, is highly suggestive of active vasculitis and therefore active disease that could be vision threatening. And so we see that in on the left side and in Panel B and Panel C. We see that that staining of multiple retinal arterioles showing that there's active disease there. In panel A, that's more consistent with perhaps retinal neovascularization, which is a consequence of of disease due to retinal ischemia, but not necessarily a sign of disease activity. And similarly, on the right side in in Panels A and C, we see this peripheral vascular staining and really more leakage that we see going on, which again is a sign of peripheral retinal ischemia, and leakage due to that, but not necessarily disease activity. Panels B and D, we see kind of this the segment of retinal arteriolar staining signs of active retinal vasculitis.
Andy Lee, MD:
So, what do you think the take home message should be for our audience in terms of young female, it's BRAO multifocal bilateral or could be any BRAO. And then they have to have imaging and hearing tests if they're symptomatic or regardless?
Drew Carey, MD:
So I think take home points, you know, if it's a single even a single branch retinal artery occlusion, that is not consistent with embolic disease, so you're not seeing it at a branch point, there's no [inaudible] there you see this segment of staining. Even in that situation, that could be the very first manifestation of Susac. So I think it's important to keep it on the differential. Certainly, if you have multiple bilateral, that's going to increase your possibility of Susac. And if they have those other classic manifestations, it certainly goes way up. But not everybody presents with all three and not everybody presents in a hyper-acute manner. So you have to keep it on your differential. And I do think because the dizziness and hearing loss in the CNS manifestations are possible. And sometimes patients are asymptomatic. Definitely in the acute presentation, the first step, you want to get all of those. And for monitoring, it is important because if they are progressing, you don't pick it up. You know, they could end up with symptomatic disease, if you can catch the preclinical hearing loss, you know, preclinical vestibular impairment, that would be important. But really the fluorescein is going to be the key for monitoring these patients. It's going to be you know, the most specific sign for disease activity and recurrence. And so we do have to have a monitoring protocol for these patients in place. And if you're a more of a neuro immunologist, with not a not a strong fluorescein background, you know, call up a friend.
Andy Lee, MD:
Well, thank you, Dr. Carey. As always, that concludes yet another edition of the NeuroOp Guru, and we'll see you guys next time.
Advertisement
Related Content
Advertisement



Latest CME


















Advertisement
Advertisement