
Commentary|Podcasts|October 15, 2025
NeuroOp Guru: When proptosis isn’t thyroid eye disease
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
Andrew G. Lee, MD, and Drew Carey, MD, highlight how chronic lymphocytic leukemia can mimic Graves’ orbitopathy, underscoring the importance of a thorough evaluation.
Advertisement






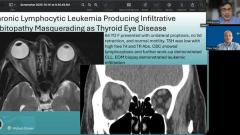


In this episode of “NeuroOp Guru” in collaboration with Ophthalmology Times, host Andrew G. Lee, MD, is joined by Drew Carey, MD, to discuss a recently published case in the Journal of Neuro-Ophthalmology highlighting a masquerade syndrome for thyroid eye disease caused by chronic lymphocytic leukemia (CLL).1 The case provides insights into the evaluation of unilateral proptosis, particularly when classic features of thyroid eye disease are absent.1
Lee is the chair of the Blanton Eye Institute at Houston Methodist Hospital and a professor of ophthalmology, neurology, and neurosurgery at the Weill Cornell Medical College. Carey is the Neil R. Miller Rising Professor of Ophthalmology in the division of neuro-ophthalmology with the Wilmer Eye Institute at Johns Hopkins University School of Medicine in Baltimore, Maryland.
Carey introduced the case: “This was a great case report in the JNO, and the authors had a patient, a 64-year-old female who presented with unilateral proptosis. The patient did not have any lid retraction and extraocular motility was normal.” Laboratory workup revealed a low TSH, elevated free T4, and positive thyroid receptor antibodies, suggesting hyperthyroidism of autoimmune etiology, likely Graves disease.1 Concurrent evaluation revealed a lymphocytosis on complete blood count (CBC), and further workup confirmed chronic lymphocytic leukemia.1
Lee and Carey noted that unilateral proptosis often raises suspicion for thyroid eye disease, given that it is the most common cause of both unilateral and bilateral proptosis. Neuroimaging initially appeared consistent with thyroid eye disease: MRI demonstrated medial rectus thickening with tendon sparing, and CT showed enlargement of multiple extraocular muscles including the superior oblique.1 Carey noted, “It looks like it’s sparing the tendons, which is very typical presentation for thyroid eye disease.”
Despite these findings, the presentation was atypical enough to warrant biopsy. Pathology revealed leukemic infiltration of the extraocular muscles, confirming that the proptosis was secondary to CLL rather than thyroid eye disease.1 Carey highlighted the importance of maintaining clinical suspicion: “Even in a patient that you think has typical thyroid eye disease and a history of hyperthyroidism and an autoimmune thyroid disease such as Graves, if they have a history of cancer, you want to be very suspicious if they’re showing up with proptosis.”
The discussion also addressed imaging and examination nuances. Carey explained that although some patients with Graves disease may have unilateral proptosis, normal motility, and absent lid retraction, these features alone do not justify routine biopsy. However, atypical features—such as the absence of lid retraction or normal thyroid antibodies—should lower the threshold for biopsy, even in patients without a known malignancy. “You should have a really low threshold for a biopsy of those patients even if they don’t have a history of cancer,” Carey said.
The episode further explored the pathophysiology of orbital involvement in leukemia. Carey noted that while the orbit lacks a formal lymphatic system, the highly vascularized extraocular muscles can serve as a site of leukemic infiltration, similar to primary ocular lymphomas.
The discussion also touched on practical clinical considerations. For patients being considered for high-dose steroids or immunosuppressive therapy, baseline CBC and attention to bone marrow status are critical. Carey noted, “Certainly, if you’re going to put somebody on high-dose steroids… you want to make sure they don’t have an active infection.”
REFERENCE
McDonald HM, Leung V, Handzic A, et al. Chronic lymphocytic leukemia producing infiltrative orbitopathy masquerading as thyroid eye disease. J Neuroophthalmol. 2025;45(2):e100-e101. doi:10.1097/WNO.0000000000002150
Advertisement
Related Content
Advertisement





Latest CME
















Advertisement
Advertisement