
Commentary|Videos|May 7, 2025
NeuroOp Guru: Eye clues that signal neuroimaging in suspected neuro-Behcet disease
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson
In cases with optic nerve hyperfluorescence or neurologic symptoms, prompt neuroimaging is warranted to rule out neuro-Behcet disease and guide multidisciplinary management.
Advertisement
Episodes in this series
EP. 2 NeuroOp Guru: Tocilizumab can have an influence on ophthalmic outcomes in giant cell arteritis
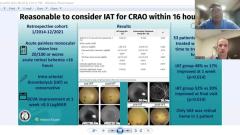
EP. 9 NeuroOp Guru: Intra-arterial thrombolysis for central retinal artery occlusion within 16 hours






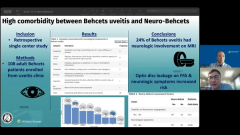


In this episode of NeuroOp Guru, Andrew G. Lee, MD, and Andrew Carey, MD, discuss the overlap between Behcet uveitis and neurologic involvement in Behcet disease, emphasizing the importance of coordinated care between uveitis and neuro-ophthalmology specialists. Behcet is a multisystem autoimmune disease that commonly affects the skin, vasculature, GI tract, and eyes. While uveitis is a hallmark finding, neuro-Behcet—though less common—is potentially life-threatening.
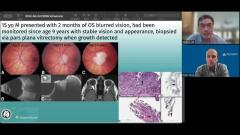
A retrospective review1 discussed in the episode examined whether ocular signs and symptoms could predict CNS involvement. Key clinical red flags included persistent headaches (especially with meningeal signs), seizures, cranial nerve deficits (eg, diplopia, facial palsy), and optic neuritis. Less common were motor and cerebellar signs; sensory or cognitive symptoms were rare.
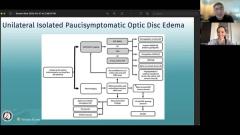
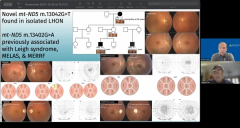
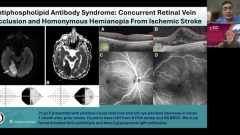
Importantly, even in the absence of overt neurologic symptoms, optic disc staining and leakage on fluorescein angiography increased the odds of neuro-Behcet (OR 5.4). This suggests that subtle optic nerve involvement seen during uveitis evaluation should prompt MRI consideration.
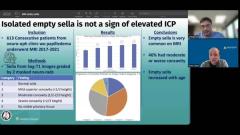
However, routine MRI for all patients with Behcet disease is discouraged due to the rarity of neuro involvement, imaging delays, and risks of incidental findings. Instead, imaging should be reserved for patients with neurologic symptoms, optic nerve signs, or high-risk fluorescein findings.
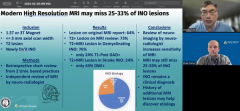
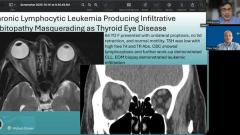
MRI findings may include venous sinus thrombosis, pachymeningitis, parenchymal enhancement, or white matter lesions mimicking multiple sclerosis. Enhancing or large white matter lesions are more concerning than age-related, non-enhancing changes.
Reference
Borelli A, Behr J, Ruggeri M, Han M, Zhou Y, Foster CS. Indications for magnetic resonance imaging in patients with Behcet uveitis. J Neuroophthalmol. 2024;44(4):473-477. doi:10.1097/WNO.0000000000002018
Advertisement
Related Content
Advertisement





Latest CME



















Advertisement
Advertisement