Now Playing

On this week's episode of the NeuroOp Guru, Andy Lee, MD, and Elizabeth Fortin, MD, discuss the current status of eye stroke evaluations for CRAO.
"...The main take home points is the current status of eye stroke evaluation has changed, and changed in a good way towards inpatient." - Andy Lee, MD
This transcript has been lightly edited for clarity:
Andy Lee, MD:
Hello, and welcome to another edition of the NeuroOp Guru. I'm here with my friend and colleague, Elizabeth Fortin and today we're going to be talking about the current status of the eyes stroke evaluation. And that is central retinal artery occlusion. So, Elizabeth, maybe you could give us a little background on why this is so important. And why do we need even know this?
Elizabeth Fortin, MD:
Yeah so, as we know, central retinal artery occlusions, is a medical emergency to the same extent other strokes are. There's been some inconsistency in their acute management over the years, for various reasons; I think there was this misconception initially that CRAOs might not be as bad, quote, unquote, as real strokes. And we know now that this is not true. And these patients really need to be managed and worked up very rapidly after the incident. And I think that's the relevance of this article. And the goal of this study was really to evaluate the practice pattern for CRAO management in one academic center over the past decade and see how it's evolved over time.
Andy Lee, MD:
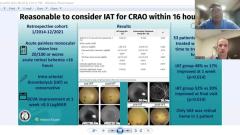
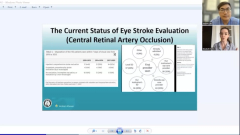
And so I think we have the table and a figure here, maybe you could just walk us through the table, and then the figure and show us what they found.
Elizabeth Fortin, MD:
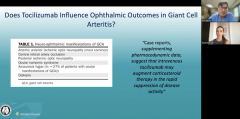
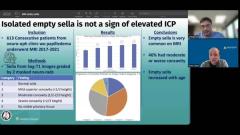
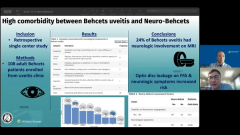
Absolutely. So there was a lot of interesting results in that study, actually. So table five is actually showing how there was a reduction. So that was one of the encouraging results, actually, because there was a reduction in the number of patients who underwent incomplete workup over time. So we see how this proportion went from 46% in between 2010 and 2013. And over time, this decreased to approximately I think, 10%, between 2017 and 2020. So this is encouraging.
There was another result that it was also encouraging, which was that the time from vision loss to presentation to the tertiary hospital actually decreased as well over the time study period, and that was also encouraging.
On the right hand side, you can see who the patients actually go to see first. 40% of patients will go to a emergency department when they have vision loss from CRAO and 50% will go to an eye provider, whether it's an optometrist, an ophthalmologist of whichever specialty so half of the patients will go to an eye doctor first.
Andy Lee, MD:
So this was just for central retinal artery occlusion, would you say the same thing applies for branch retinal artery occlusion?
Elizabeth Fortin, MD:
Absolutely, branch retinal artery occlusion, CRAOs, even amaurosis fugax — so transient monocular blindness — should also go into the same category.
Andy Lee, MD:
Does it matter whether we see the embolus or not?
Elizabeth Fortin, MD:
It doesn't matter. The embolus can disappear over time; it's possible that it was blocked at one point in the vessel and moved through the vessel and now we can't see it. So it doesn't matter if we can see it or not. I think we have to treat these patients with the same level of emergency, which is very urgent, whether we see the embolus or not.
Andy Lee, MD:
And so what if it's one day old, go to the stroke service? One day?
Elizabeth Fortin, MD:
Yes, I think yes. And I don't know if this is how you practice, but I think if you see the patients within the first probably week or a couple of weeks, it's very important that they get worked up acutely. And this is because it changes their prognosis, they're at risk of having another stroke within the next couple of weeks. And they also can benefit from treatment. If they have, for example, severe carotid disease, they benefit from an earlier treatment within seven days if they're seen acutely. So I think it's very important.
Andy Lee, MD:
So you're not really doing it to get their vision back. You're doing it for the stroke workup.
Elizabeth Fortin, MD:
Now we're doing it for the stroke workup. But hopefully over time through patients education and eye care provider — or any provider — education, we can get the patients in early and we can actually see if potential treatments would be beneficial for visual recovery. But the issue right now is we have trouble getting the patients to tertiary centers rapidly enough. We have to see them within five hours, probably four and a half hours, for them to benefit from any treatment with thrombolysis. So I think we have trouble getting down to that timeframe. And that's what we have to work on for the next several years.
Andy Lee, MD:
What about if it's two weeks?
Elizabeth Fortin, MD:
This is a very good question. And I would like to ask you, because, you know, if it's two weeks, three weeks, is it reasonable to get it in a timely matter? I would still try to get the workup done within probably a week or two. Can it be done as an outpatient? It depends where you live, I think, and if you can get the workup done rapidly enough. I wouldn't still wait several weeks or months to get these workup done. What do you think about that?
Andy Lee, MD:
So if it's two hours or two days, or two weeks, they're coming to the hospital; two months, we let the stroke service tell us whether they have to come to the hospital. And often they can do an expedited workup for the two month person. If it's two years, or two decades, you can't do nothing with that, and usually, it's way too late and whatever bad thing already happened, and they probably don't have a treatable stroke respecter.
So I kind of use that as a rough guideline. But that borderline, as you said, we let stroke service make the call for all of these I don't I don't try and be the limiting factor on whether stroke should admit or not, I let them choose. And as you said, individual practices and individual variations vary from place to place. And so I don't think it's our role to make that decision. We just make the call to the person that makes that call.
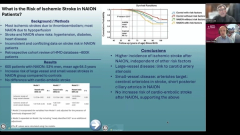
How about stroke in the eye if it's NAION, does that need to come into the hospital? Is that in the eye?
Elizabeth Fortin, MD:
No. So that's a good, very good interesting point because NAION is not an embolic event the wide variety of the cases, there are a few exceptions, but most commonly not. So these patients don't need to be admitted to the hospital. So this is a very different type of eye stroke. I wish we didn't call it really eye stroke in that situation because it gets confusing. I think CRAOs, BRAOs are eye stroke, NAION isn't really.
Andy Lee, MD:
Yeah, so I think that's really the main take home points is the current status of eye stroke evaluation has changed, and changed in a good way towards inpatient. There are less people being worked up inappropriately as an outpatient or incompletely or not at all, which is a great thing that they have noted. And that there is a difference between eye stroke layperson version, ischemic optic neuropathy, and what we consider a real stroke of the eye, which is retinal artery occlusions.
And I agree, we do not admit NAION — nonarteritic anterior ischemic optic neuropathy — I consider that to be a small vessel ischemic event, not an eye stroke. And what's very scary, but also very important is the first provider seen is often the outside eye care provider and stroke of the eye needs a stroke workup at the stroke center by the stroke doctor. And the timing of that stroke workup probably should be made by the stroke doctor and not by us.
There any other last message you want to leave our audience with Elizabeth on the current status of eye stroke evaluation?
Elizabeth Fortin, MD:
Well, I think I completely agree with what you just said. I think there are two things we can work on: patient education, but also eye care provider education to make sure that these patients get to the hospital as fast as possible.
Andy Lee, MD:
And that concludes another edition of the NeuroOp Guru. Thanks, Elizabeth, for participating and I'll see you guys next week.