
|Videos|March 23, 2023
NeuroOp Guru: Unilateral isolated paucisymptomatic optic disc edema - what is that?
Author(s)Andrew G. Lee, MD, Elizabeth Fortin, MD
On this week's episode of the NeuroOp Guru video blog, Andy Lee, MD, and Elizabeth Fortin, MD, discuss unilateral isolated paucisymptomatic optic disc edema and what exactly it is.
Advertisement
Episodes in this series
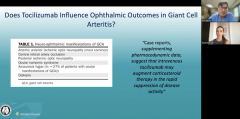
EP. 2 NeuroOp Guru: Tocilizumab can have an influence on ophthalmic outcomes in giant cell arteritis
Now Playing
EP. 7 NeuroOp Guru: Unilateral isolated paucisymptomatic optic disc edema - what is that?








Andy Lee, MD:
Hello and welcome to another edition of the NeuroOp Guru. I'm here with my good friend Elizabeth. Hi, Elizabeth. And today we're going to be talking about unilateral isolated paucisymptomatic optic disc edema. What is that?
Elizabeth Fortin, MD:
This is basically when you see a patient that has unilateral disc edema that's either asymptomatic completely or that has very minimal visual symptoms.
Andy Lee, MD:
And so what was the author's contention here in terms of do we have to work it up? Or can we just follow it, and do we have to image it.
Elizabeth Fortin, MD:
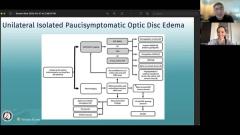
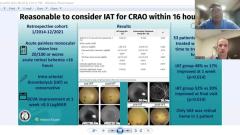
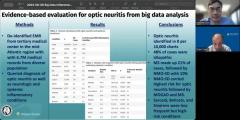
So the authors in this article reviewed 29 patients that presented with the unilateral optic disc edema with barely no symptoms. And, you know, they ended up finding that most of these patients had said diagnosis that they could make after doing a thorough evaluation and diagnostic workup. Only 4 patients ended up with the diagnosis of exclusion that we've all heard about that is papillophlebitis. And we can talk a little bit more about what papillophlebitis is, but the other patients were all found to have other diagnoses such as increased intracranial pressure, or meningiomas or orbital masses. So definitely, these patients need to be worked up thoroughly in order to find a cause for their optic disc swelling, and also to avoid vision loss in the future if they have a definitive diagnosis.
Andy Lee, MD:
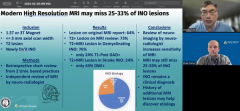
So I think I agree with the imaging. And do you think we have to have MR venogram for unilateral disc edema, that because it might be unilateral papilledema?
Elizabeth Fortin, MD:
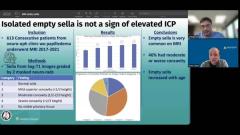
Yeah, so that's, that's the rationale of what why was obtained there. You know, you could debate that if the patient is completely asymptomatic and doesn't have particular risk factors. So it's just for example, smoking, you could probably start with just an MRI brain and orbits within without contrast. But I think it's reasonable to add it if you were to find some signs of increased intracranial pressure, and you're not sure about the diagnosis. But that would be, you know, surprising, and none of the patients in the article were found to have Venous Sinus Thrombosis, were all found to have Idiopathic Intracranial Hypertension. But I still think that there's it's very important to obtain brain image and brain orbit imaging and these patients, actually, all of the patients, except for 1 in this study, obtain good high quality MRI imaging.
Andy Lee, MD:
And how about lumbar puncture? Would you do it? If you had no symptoms and no radiographic signs of increased intracranial pressure?
Elizabeth Fortin, MD:
I think this, you probably don't need to obtain a lumbar puncture. In these situations. It's again, you could debate you know, in this study, the patients who obtain lumbar puncture all had signs of increased intracranial pressure on the MRI. And that's what led to doing the performing the lumbar puncture. If you know you're going to have you know, a follow up with the patient and you're not going to lose them to follow up, I think it's reasonable to hold back on that lumbar puncture. What's your opinion on that?
Andy Lee, MD:
So I tell the patient that if they have no symptoms and clinically and no radiographic features of increased intracranial pressure, that we follow them, but if the disc edema doesn't go away, I do do a lumbar puncture. But if it goes away, or I can make a plausible alternative diagnosis, and there's that long list there on the side of vitreopapillary traction or incipient NAION or disc drusen related NAION or papillophlebitis, whatever that is, if I feel comfortable with any of those other ocular diagnoses, then I don't do a spinal tap. But the chronic people and the people, I can't pin it on NAION or some other cause I do do a spinal tap, even if it's unilateral. Most of those cases I have found to be asymmetric, but bilateral not truly unilateral. There was always something like funny about the other optic nerve, but maybe it can be both.
Elizabeth Fortin, MD:
Yeah, I agree with that.
Andy Lee, MD:
How about fluorescein? Are you doing fluorescein angiogram on every single person?
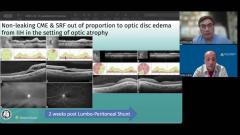
No, I think you have to use your clinical judgment and look at the aspect of the disc swelling as well. I think fluorescein is used when you have suspicion of maybe a oculal CRVO or when you have vascular changes in the retina or some features like that, like tortuosity of the vessels and it can help you confirm for example, an impending CRVO but I don't do it on every patient.
Andy Lee, MD:
I'm the same way. And I think that's why the authors have that plus/minus there where they're kind of hedging on those 2 tests.
Yes, exactly.
Andy Lee, MD:
So I think vitreopapillary traction that one's kind of easy the OCT can see that. CRVO, I think that's kind of easy to even the incomplete ones? Drusen, probably easier also. How about papillophlebitis, diabetic papillopathy and incipient NAION, how would you say those have to be diagnosed?
Elizabeth Fortin, MD:
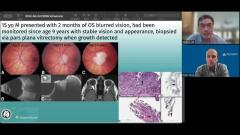
So the article is, is really good in explaining the whole history behind papillophlebitis. I think it's a confusing term just because it's been used for different conditions in the past, right. So some patients were described as having papillophlebitis probably actually had a mild version of CRVOs. So I think in the end, what you can call papillophlebitis, and the term might be wrong, because it implies that maybe you have an inflammatory component to it, although it's never been shown in the pathologic assessment of these patients. But patients you will categorize in papillophlebitis are probably young patients below the age of 50, without any vascular risk factors, will present chronic optic disc edema with no symptoms, and can have peripapillary vascular changes and vascular tortuosity of the veins, but not in the periphery. Because if you think of patients that have peripheral hemorrhages, you should probably call these patients impending or mild CRVOs. So I think that's the confusion with these people. And they often evolve very well right, don't end up with any visual loss in the future, but the swelling can last for several years.
Andy Lee, MD:
So what would be your bottom line take home message if you are counseling our listeners on unilateral, isolated either paucisymptomatic or asymptomatic optic disc edema.
Elizabeth Fortin, MD:
I think you have to do a very thorough exam and diagnostic workup for these patients because I think what this article shows is that in most cases, you will find a cause for the unilateral disc swelling and in some cases, you can prevent some vision loss in the future such as patients that have maybe tumor or orbital masses or meningioma. So, it's important to be careful with these patients. And if you don't have a very clear ocular reason for the optic disc edema, you should work them up with brain imaging and or lumbar puncture as well.
Andy Lee, MD:
Well, that concludes yet another edition of the NeuroOp Guru and I thank you, Elizabeth for your time and attention and advice. I'll see you guys next week.
Elizabeth Fortin, MD:
Thank you
Advertisement
Related Content
Advertisement




Latest CME






















Advertisement
Advertisement