
Commentary|Podcasts|October 28, 2025
NeuroOp Guru: Live from AAO 2025
Author(s)Andrew G. Lee, MD, Andrew Carey, MD
Fact checked by: Sheryl Stevenson, Sydney M Crago
Andrew G. Lee, MD, and Drew Carey, MD, discuss the case of a patient with persistent papilledema after brain tumor resection due to superficial siderosis.
Advertisement








Andrew G. Lee, MD, was joined by Drew Carey, MD, for a live recording of the Ophthalmology Times “NeuroOp Guru” during the American Academy of Ophthalmology 2025 annual meeting, held October 18-20, in Orlando, Florida. They discussed an instructive case of superficial siderosis and chronic papilledema following brain tumor resection.1
The case centered on a patient with glioblastoma multiforme (Grade 4) who underwent 3 surgeries.1 Postoperatively, the patient in this case noted, “Doctor, my vision’s going dark,” Carey summarized. Neuro-ophthalmologic evaluation revealed bilateral optic disc swelling but “no more brain tumor.” MRI revealed diffuse hemosiderin deposition across the cerebellum, consistent with superficial siderosis.1
As Carey explained, “Superficial siderosis is usually a condition caused by a chronic bleed in the head,” though it may also result from episodic bleeding. The iron deposition in the subpial layers can “restrict CSF reabsorption,” predisposing patients to elevated intracranial pressure and papilledema. While progressive sensorineural hearing loss and cerebellar ataxia are the hallmark features, papilledema, though less common, can occur when “CSF reabsorption is impaired by that hemosiderin deposition.”
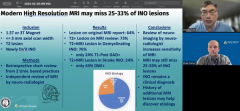
Importantly, the diagnosis often requires advanced imaging. “We can’t just see this on a regular MRI,” Carey noted. “You kind of need the special sequence.” For detection, “the original ones are T2 GRE,” though “more commonly we’re using susceptibility-weighted imaging,” both of which enhance visualization of hemosiderin, he said.
The discussion closed with a key reminder for ophthalmologists: “If your patient had a brain tumor and they had surgery and they had papilledema beforehand, you still need to see them afterwards,” Carey said. Persistent or recurrent papilledema may signal postoperative complications such as superficial siderosis or CSF flow impairment, not necessarily tumor recurrence. As Carey emphasized, “don’t be afraid to reimage your cancer patients who have swollen optic nerves.”
This case underscores the importance of vigilant postoperative surveillance, targeted imaging, and multidisciplinary management in patients with complex neuro-ophthalmic sequelae of brain tumor surgery.1
REFERENCE
Spiegelman DV, Stunkel L, Goyal MS, et al. Superficial siderosis causing refractory papilledema following brain tumor resection. J Neuroophthalmol. 2025;45(2):e142-e144. doi:10.1097/WNO.0000000000002178
Advertisement
Related Content
Advertisement





Latest CME



















Advertisement
Advertisement