






















Error in first eye can guide decisions in IOL selection for fellow eye of patients
Error in first eye can guide decisions in IOL selection for fellow eye of patients

Study finds similar results for patients who received hydrophobic, hydrophilic acrylic lenses

Robin R. Vann, MD, and Douglas D. Koch, MD, discuss the nuances of the procedure
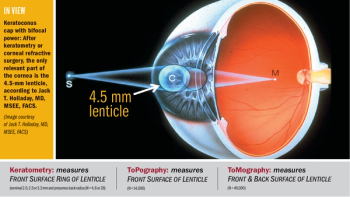
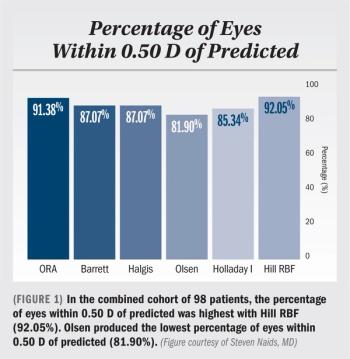
Pearls for overcoming pitfalls related to keratometry, prediction of effective lens position, optical biometry

Laser technology has potential to modify IOL refractive index without change to lens shape

Approach aids toric IOL alignment, IOL centration, wound/astigmatic keratotomy placement

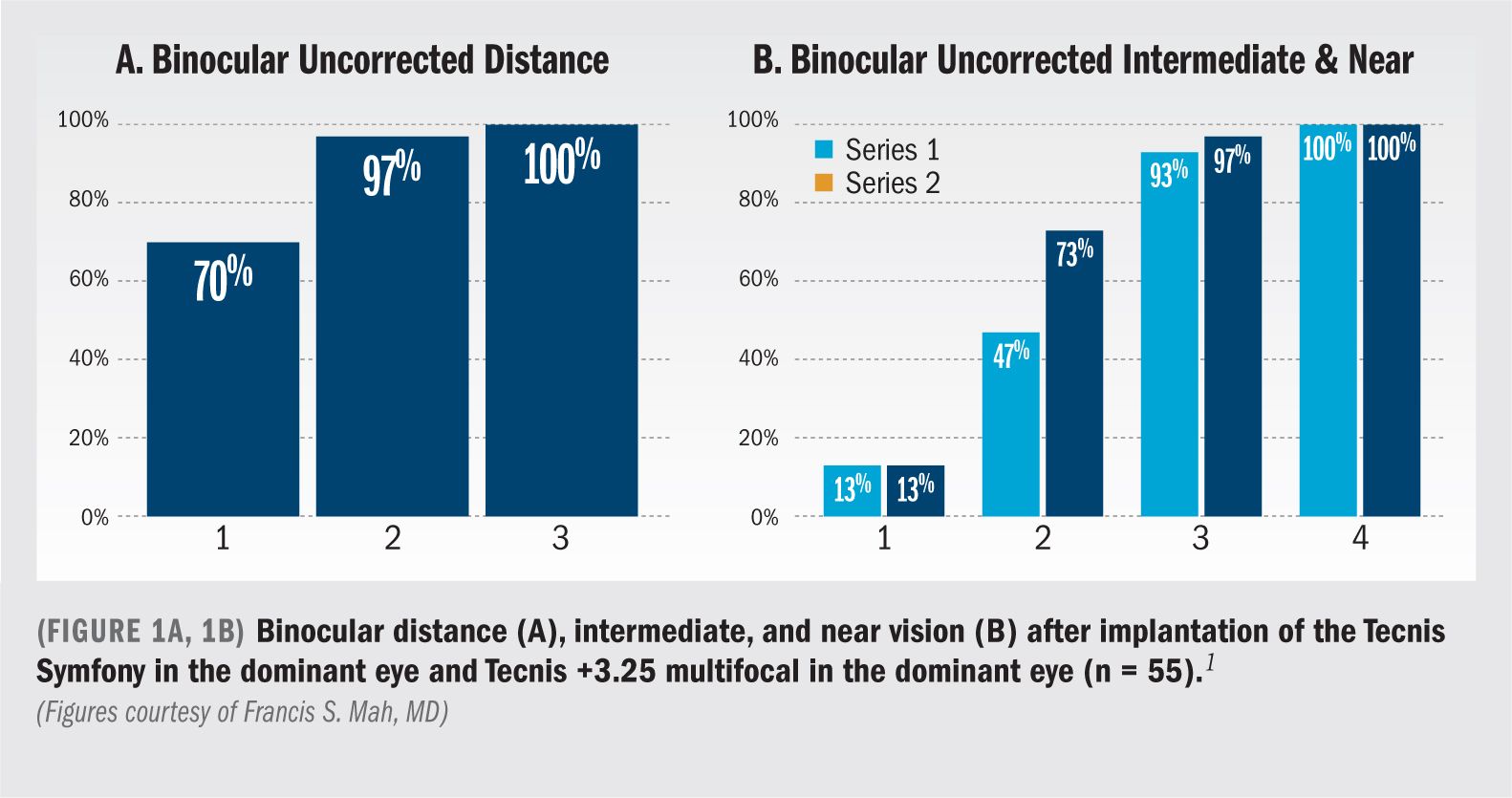
Medium-add multifocal addresses the most likely source of dissatisfaction with contemporary multifocal IOLs: Intermediate vision



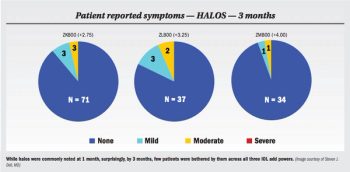
In a well-matched sample group, patients with higher levels of postoperative astigmatism reported a greater improvement in quality of life and a greater rate of willingness to have the procedure again if they received an Extended Depth of Focus IOL compared to patients receiving a low-add, multifocal IOL, despite similar postoperative clinical and patient reported performance.
Findings from a pilot study show that a novel accommodative intraocular lens (AIOL, Lumina, Akkolens) provides a true accommodative response that is maintained for at least 2 years and preserved following Nd:YAG laser capsulotomy.
Surgeons work hard to get happy patients, and satisfied patients spread the word and refer their friends. They don't need extra post-op visits, and can return yearly to see their referring doctor. Selecting the best presbyopia-correcting IOL for a patient is critical and depends on methodical, preoperative decision-making.
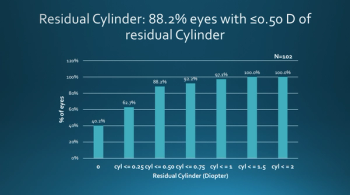
Findings of a study determining the prediction error in the magnitude of residual astigmatism after cataract surgery with a toric intraocular lens (IOL) suggest that use of intraoperative wavefront aberrometry for toric power selection could enhance the refractive outcome in a large subset of eyes.
A prototype of a novel dual-mode, accommodating-disaccommodating intraocular lens with zonular capture haptics has been fabricated successfully. The lens has shown in bench studies to exhibit axial shift and shape change that results in up to about 26 D of accommodative change,
Steven Vold, MD, reports that toric IOLs provide an accurate, safe, and convenient way to correct astigmatism and uncorrected distance vision for glaucoma patients, while patients wanting presbyopic correction have IOL options to fit a range of visual needs.