Publication
Article
Digital Edition
Keratoconus management: Lessons learned from an unusual time
Author(s):
Timely access to effective diagnosis and cross-linking is key to positive outcomes


Delays in diagnosis and treatment are not uncommon even without a pandemic, and the need for preauthorization and other insurance-related delays continue to be the most common barrier to timely treatment.

As 2022 comes to a close, we all hope the SARS-CoV-2 virus will have a limited impact on patient care this winter and in the years to come. We know that ophthalmic care was dramatically affected in the early days of the pandemic.
Nearly all practices closed in March and April 2020, providing only urgent and emergency care. In our practice and in most settings, cross-linking surgery for keratoconus (KC) was not considered an urgent or emergency procedure. The relatively long duration of the procedure, during which the patient is in close contact with the physician and staff, led many to consider it too risky to perform at the beginning of the pandemic.
Even as practices reopened and began performing cross-linking again, there were significant delays in care. In many cases, patients were reluctant to come to medical facilities, fearing exposure to the virus. I still occasionally see a patient with a diagnosis of KC who has not been evaluated since before the pandemic. The most significant factor for delayed care was probably the delay in new KC diagnoses, as patients postponed and failed to reschedule routine eye care visits where an optometrist might have noticed unusual keratometry, rapidly changing astigmatism, or other red flags.
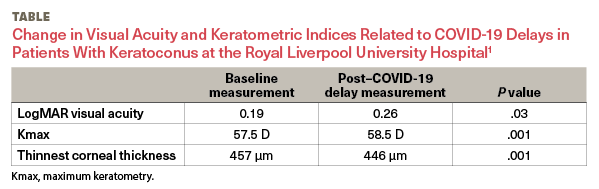
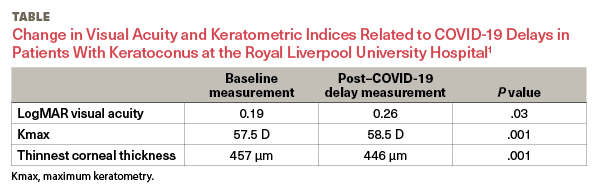
Several papers have looked at the impact of altered patterns of care during the pandemic on KC management and outcomes, with some important lessons for us all. First, delays in care have a negative impact on patient outcomes. Shah et al found there was an average delay of 6 months in treatment for patients who were about to be scheduled for cross-linking at the start of the pandemic. Of these 6 months of delay, approximately 3 months were due to service suspensions related to COVID-19.1 As a result of this delayed treatment time period, patients in the study lost an average of 1 line of visual acuity (Table1). Depending on which clinical criteria were used to measure progression, 39% to 70% of patients exhibited further progression of KC due to these delays.1
We know that delays in diagnosis and treatment are not uncommon even without a pandemic. Patients have busy lives and other health issues; they may put off a recommended specialist consultation, especially if they live outside metropolitan areas where most cornea specialists practice. School-aged patients may postpone cross-linking until a school year ends. And despite improvements in insurance reimbursement for cross-linking, the need for preauthorization and other insurance-related delays continue to be the most common barrier to timely treatment.
Second, the pandemic studies reinforce that focusing on younger patients, who are most likely to exhibit rapid progression,2 is essential. At a center in Lombardy, Italy, one of the earliest epicenters of the pandemic, doctors prioritized rescheduling by the severity of KC risk and patients’ risk factors for COVID-19.
Younger patients with progressive KC who had not yet undergone cross-linking or whose second eye was affected after cross-linking on the first eye and who had no comorbidities related to elevated COVID-19 susceptibility were deemed the highest priority. Ultimately, the department accelerated treatment in 50% of these younger patients with KC based on documented evidence of KC progression.3 This is a good reminder that teenaged patients and patients aged in their 20s should be followed very closely—perhaps as often as every few months—because they can experience progression even in that short period of time.
Finally, we learned that in-person evaluation of patients for KC remains critical to accurate diagnosis and cannot easily be replaced. In one study, researchers found that patients with KC enrolled in a virtual care model during the summer of 2020 were overwhelmingly satisfied with it.4 However, another study found that telehealth visits could not accurately detect KC progression as well as the gold-standard in-person visit.5 In that study, researchers found that although remote assessment had a high level of specificity (96%), there were many false negatives, resulting in a relatively low sensitivity rate (69%).
I have been performing cross-linking for about 10 years, first in clinical trials and then in a commercial setting since approval of the iLink system. As a treatment that can prevent further progression, cross-linking is an essential tool in the management of progressive KC, especially for younger patients for whom the opportunity to prevent vision loss and avoid a corneal transplant can be life-changing. These studies from the COVID-19 era should serve as an important lesson in the value of timely access to effective diagnosis and cross-linking.
Audrey Talley Rostov, MD
E: atalleyrostov@nweyes.com
Rostov is a partner at Northwest Eye Surgeons in Seattle, Washington, and serves as a board member and medical liaison for SightLife. She is a consultant for Glaukos.

References
1. Shah H, Pagano L, Vakharia A, et al. Impact of COVID-19 on keratoconus patients waiting for corneal cross linking. Eur J Ophthalmol. 2021;31(6):3490-3493. doi:10.1177/11206721211001315
2. Romano V, Vinciguerra R, Arbabi EM, et al. Progression of keratoconus in patients while awaiting corneal crosslinking: a prospective clinical study. J Refract Surg. 2018;34(3):177-180. doi:10.3928/1081597X-20180104-01
3. Legrottaglie EF, Balia L, Camesasca FI, et al. Management of an ophthalmology department during COVID-19 pandemic in Milan, Italy. Eur J Ophthalmol. 2021;31(5):2259-2267. doi:10.1177/1120672120960334
4. Iselin KC, Kaufmann C, Malata D, et al. Telemedicine service for keratoconus monitoring: patient satisfaction and prospects for further expansion. Telemed J E Health. Published online April 14, 2022. doi:10.1089/tmj.2021.0619
5. Barequet D, Gutfreund S, Goldstein M, Loewenstein A, Gamzu R, Varssano D. Evaluation of a telemedicine model for following keratoconus patients in the era of COVID-19 pandemic. Telemed J E Health. 2022;28(7):1023-1027. doi:10.1089/tmj.2021.0178











Newsletter
Don’t miss out—get Ophthalmology Times updates on the latest clinical advancements and expert interviews, straight to your inbox.
 NeuroOp Guru: Using OCT to forecast outcomes in ethambutol optic neuropathy")
 Inside NYEE’s new refractive solutions center with Kira Manusis, MD")
 Dilsher Dhoot, MD, on the evolution of geographic atrophy therapy: where are we now?")
 Anat Loewenstein, MD, shares insights on the real-world results of remote retinal imaging")
 Two-wavelength autofluorescence for macular xanthophyll carotenoids with Christine Curcio, PhD")
 FLIO and the brain: Making the invisible visible with Robert Sergott, MD")
 Structure-function correlates using high-res OCT images with Karl Csaky, MD, PhD")
 SriniVas Sadda, MD, on high-res OCT of atrophic and precursor lesions in AMD")
 Christine Curcio, PhD, shares histology update supporting review software and revised nomenclature for <3 μm OCT")
 ASCRS 2025: Eric D. Donnenfeld, MD, on the effect of lifitegrast clinical signs and biomarkers in dry eye disease")