
Two-year results of laser scleral microporation
Procedure can reduce scleral biomechanical stiffness and rejuvenate dynamic range of focus.

")
(Image Credit: AdobeStock/ribalka yuli)

With age and the onset of presbyopia, several things are happening at once. The crystalline lens is undergoing changes in size, shape, and flexibility. At the same time, the sclera is becoming stiffer from an age-related accumulation of advanced glycation end products, resulting in cross-linking of collagen microfibrils.1 Zonular tension may also be altered. Together, these changes lead to a loss of the ciliary muscle force needed to adjust the lens during accommodation. The exact timing and interaction of all these age-related changes are not yet fully understood, but we certainly know the outcome: loss of the eye’s dynamic range of focus (DROF) and increasing difficulty with near and intermediate tasks.
A new treatment approach
Laser scleral microporation (LSM) is an investigational treatment with the potential to reverse the effects of aging on the sclera, softening it and restoring natural biomechanical movement of the ciliary muscles and lens. After porcine and primate proof-of-concept studies demonstrated good results,2,3 a 2-year clinical pilot study was conducted at my clinic in Manila, Philippines.4


Figure 1: In the laser scleral microporation procedure, a matrix of scleral micropores is created in 4 oblique quadrants outside the visual axis.
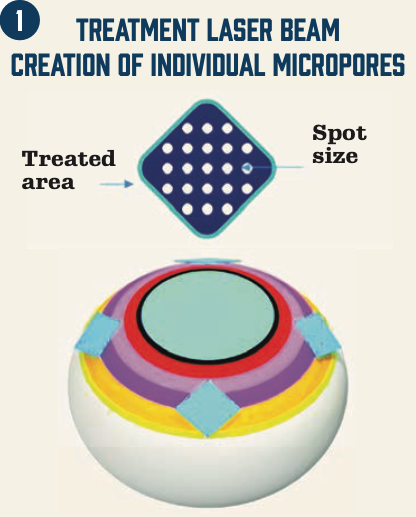


Figure 2: The microporation matrix can be seen under surgical microscopic magnification but is not visible without magnification.

In the LSM procedure, a 2.94-µm Er:YAG laser (VisioLite, ACE Vision Group) is used to create a diamond-shaped matrix of transconjunctival scleral micropores in 4 oblique quadrants of the sclera (Figure 1 and Figure 2), well outside the visual axis. Each matrix is 5.0 x 5.0 mm and comprises a series of 225-µm micropores that can be delivered simultaneously by the laser at a depth of 85%. Treating 4 quadrants, rather than 360° around the sclera, avoids the large blood vessels and nerves entering the eye at approximately 2, 4, 7, and 10 o’clock. Each quadrant takes less than 15 seconds to treat, with a total treatment time of about 10 minutes for both eyes. LSM is performed over 5 critical anatomical zones over the ciliary muscle and other extralenticular structures of the accommodative apparatus.4 LSM is designed to be performed bilaterally so that both eyes can subsequently focus for natural binocular vision. Because this noninvasive, extraocular procedure does not penetrate the sclera or the cornea, it can be performed as an in-office procedure.
Clinical study results
In the 2-year pilot study, 100 eyes of 50 patients with emmetropia and presbyopia were treated with the LSM procedure.5 To be enrolled, patients had to have uncorrected near visual acuity of 20/50 or worse, less than 1.0 diopter (D) of astigmatism, and a manifest refraction within 0.50 D of emmetropia, with good stereopsis. Patients with cataracts, dry eye, or prior ocular surgery were excluded. After LSM, the patients were treated with prednisolone 4 times a day for 2 weeks, moxifloxacin 4 times a day for 1 week, and artificial tears as needed. They were instructed to avoid using reading glasses to allow for reengagement of the ciliary muscle.
The patients were majority female (70%), with a mean age of 56.6 years and a mean reading add of 2.00 D. Initial results demonstrate that throughout 2 years of follow-up, patients experienced significant improvements in distance-corrected and -uncorrected (Figure 3) near and intermediate visual acuity, measured at 40 cm and 60 cm, respectively, with no change in distance vision. Although there was some variability in the response, most patients achieved near-vision improvements within the first week, with continued improvement through month 3 and stability between 3 and 6 months and sustained over 24 months. There were no complications in the study other than occasional subconjunctival hematoma, which resolved within 2 weeks. We saw a statistically significant decrease of 2.7 mm Hg (19%) in these normotensive eyes.
Patients completed the Near Activity Visual Questionnaire at multiple time points to assess visual task performance and overall satisfaction.6 The summed Rasch score, indicating difficulty with near-task performance, dropped significantly from 64.68 at baseline
to 38.70 at 24 months (P <.05). About three-quarters of patients (73%) reported moderate to complete satisfaction with their near vision. The patient-reported improvement in reading ability, mirroring the visual acuity gains, was achieved by 3 months and was stable through the 24-month visit. Most patients did not need readers for most tasks after the treatment and told me anecdotally that they no longer experienced headaches when trying to focus at near.

")
Figure 3: Binocular uncorrected vision following laser scleral microporation. (Images courtesy of Robert T. Ang, MD)

There are a number of advantages to the LSM procedure. It is relatively quick and easy to perform. The patient experience is a very positive one, with no pain or unwanted adverse effects. And unlike all other presbyopia treatments now available on the market, LSM does not affect distance vision. Patients do not have to sacrifice distance acuity or quality because the treatment is outside the visual axis.
Future research directions
Data collection in this study is continuing, and we have much still to learn about LSM, including more about its duration of effect, which factors predict an optimal result, the repeatability of the procedure, and how best to combine it with other presbyopia treatments or refractive corrections.
Thus far, I am enthusiastic about the potential for LSM to reduce scleral biomechanical stiffness and rejuvenate the natural DROF.



Robert T. Ang, MD
E: angbobby@hotmail.com
Ang is a senior consultant and head of Cornea and Refractive Surgery Services at the Asian Eye Institute in Manila, Philippines. He is a consultant for Ace Vision Group Inc. AnnMarie Hipsley, DPT, PhD, and Mitchell A. Jackson, MD, were coauthors of the study.
References:
1. Schultz DS, Lotz JC, Lee SM, Trinidad ML, Stewart JM. Structural factors that mediate scleral stiffness. Invest Ophthalmol Vis Sci. 2008;49(10):4232-4236. doi:10.1167/iovs.08-1970
2. Ting DSJ, Liu YC, Price ER, et al. Improvement in accommodation and dynamic range of focus after laser scleral microporation: a potential treatment for presbyopia. Transl Vis Sci Technol. 2022;11(12):2. doi:10.1167/tvst.11.12.2
3. Liu YC, Hall B, Lwin NC, et al. Tissue responses and wound healing following laser scleral microporation for presbyopia therapy. Transl Vis Sci Technol. 2020;9(4):6. doi:10.1167/tvst.9.4.6
4. Knaus KR, Hipsley A, Blemker SS. The action of ciliary muscle contraction on accommodation of the lens explored with a 3D model. Biomech Model Mechanobiol. 2021;20(3):879-894. doi:10.1007/s10237-021-01417-9
5. Shah S. Dynamic range of focus recovery after laser scleral microporation in emmetropic presbyopes: 24 month pilot study outcomes. British Society for Refractive Surgery, 2023.
6. Buckhurst PJ, Wolffsohn JS, Gupta N, Naroo SA, Davies LN, Shah S. Development of a questionnaire to assess the relative subjective benefits of presbyopia correction. J Cataract Refract Surg. 2012;38(1):74-79. doi:10.1016/j.jcrs.2011.07.032

























