For younger patients with midrange myopia, consider phakic IOLs
The implantable lenses can offer an advantage over laser surgery.

")
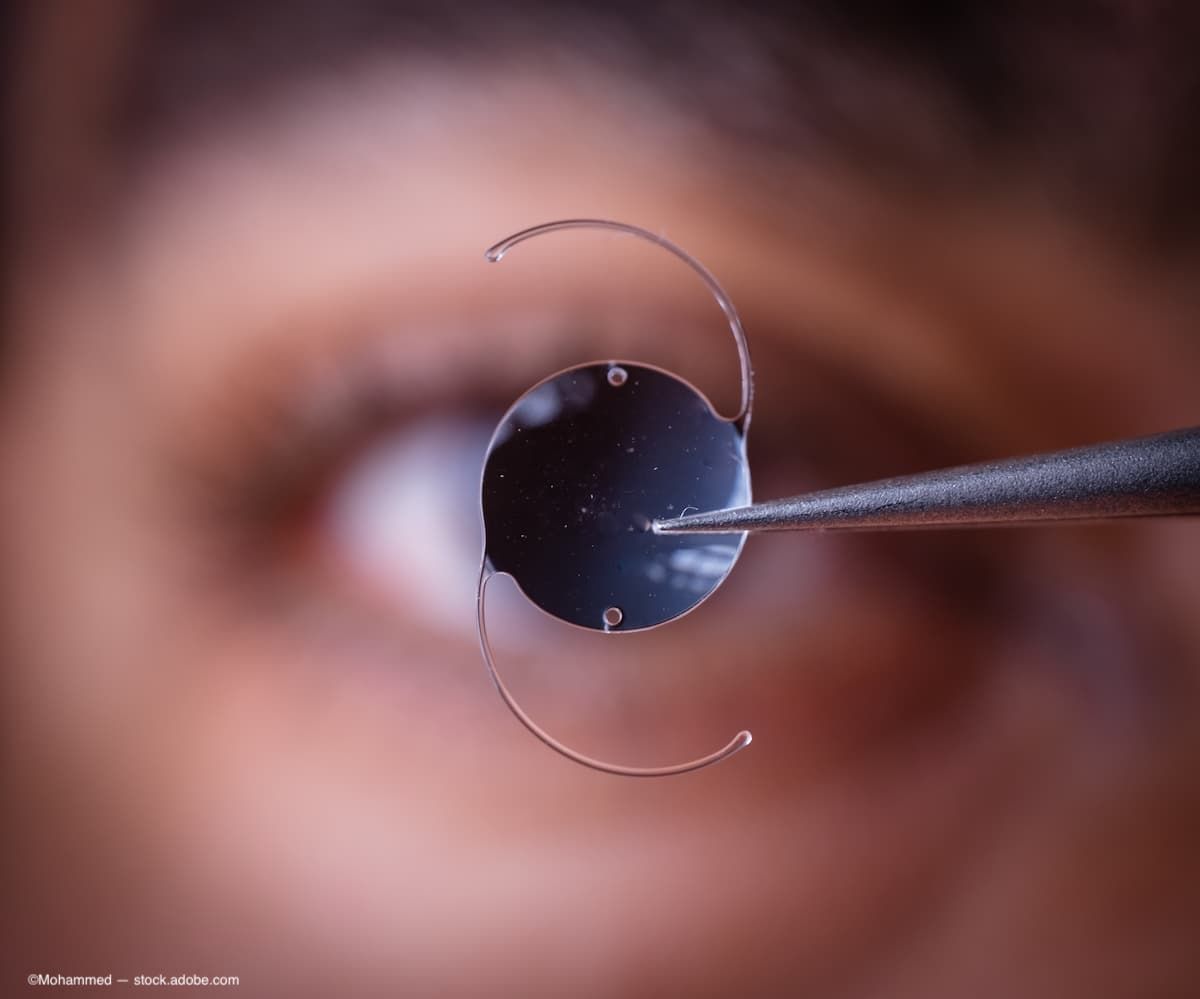
(Image Credit: AdobeStock/Mohammed)
As a specialist in refractive surgery, I regularly treat younger adults with midrange myopia who dream of waking up every morning and enjoying 20/20 vision without having to grapple with glasses or contact lenses.
For many of these patients, one of my first recommendations is a strategy that other ophthalmologists often use only when laser in situ keratomileusis (LASIK) is contraindicated: phakic IOLs, which are implanted behind the iris through a tiny corneal incision, leaving the eye’s natural lens in place to facilitate focusing at multiple distances. In fact, having launched a new practice this year, I will be positioning this game-changing approach as the cornerstone of my menu of services, helping to distinguish my business among our region’s more traditional refractive clinics. The goal for Mueller Vision is to serve as a comprehensive refractive surgery practice that is able to offer the best technologies and procedures for each individual patient.
I have no doubt that my patients will appreciate the chance to consider these implantable lenses. Perhaps because they sit so close to the eye’s nodal point, there is evidence that phakic IOLs sharpen vision more effectively than laser surgery compared with baseline values corrected by glasses or contact lenses. Many patients even gain a line of vision on an eye chart.1 Another advantage is that these lenses represent the only reversible refractive procedure, meaning that they can easily be removed by a doctor if additional surgeries become necessary due to life stage–related vision changes—eg, presbyopia or cataracts.
As a subinvestigator in an FDA pivotal clinical trial of a recent phakic lens technology,2 I have seen the excellent outcomes this approach can bring. Also, I have been pleased to receive excellent feedback from patients who have undergone the procedure in my clinic.
Due to the many benefits of this technology, the time has come for ophthalmologists to consider phakic IOLs as a first-line approach in younger adults seeking a fix for their midrange myopia.
The advantages of phakic IOLs
In my practice, my main goal is to get patients out of glasses or contacts. So for those eligible for either LASIK or phakic IOLs, I don’t typically recommend one strategy over the other, as both will safely, significantly, and reliably improve vision compared with baseline measurements seen with glasses and contacts. Rather, I speak to my patients about every available option before helping them pick procedures based not only on their medical eligibility but on the factors they consider most important—from the mechanics of the procedures to anticipated outcomes, including postsurgical suitability for treatments that may be needed for presbyopia or cataracts in the future.
When choosing between these 2 surgeries, a few pros and cons deserve discussion:
Reversibility
The unique reversibility of a phakic IOL procedure offers an advantage over other refractive surgery types, as there are several reasons patients might want to remove the lenses as their vision changes across many decades.
Over a lifetime, the eyes hit 3 ocular milestones:
- Ocular maturity, which occurs between the ages of 18 and 21 years, when the eyes stop growing and changing, leading to a period until about age 40 that is often marked by treatment for myopia or astigmatism;
- Presbyopia, which occurs when patients enter their 40s; and
- Cataracts, which typically need treatment after the age of 65.
Although LASIK is both appropriate and effective at ocular maturity, it makes permanent changes to the cornea, leaving patients ineligible for some of the presbyopia treatments they might otherwise consider later in life.

")
A lateral view of how an EVO is positioned in the eye. (Image courtesy of Brett Mueller II, DO, PhD)
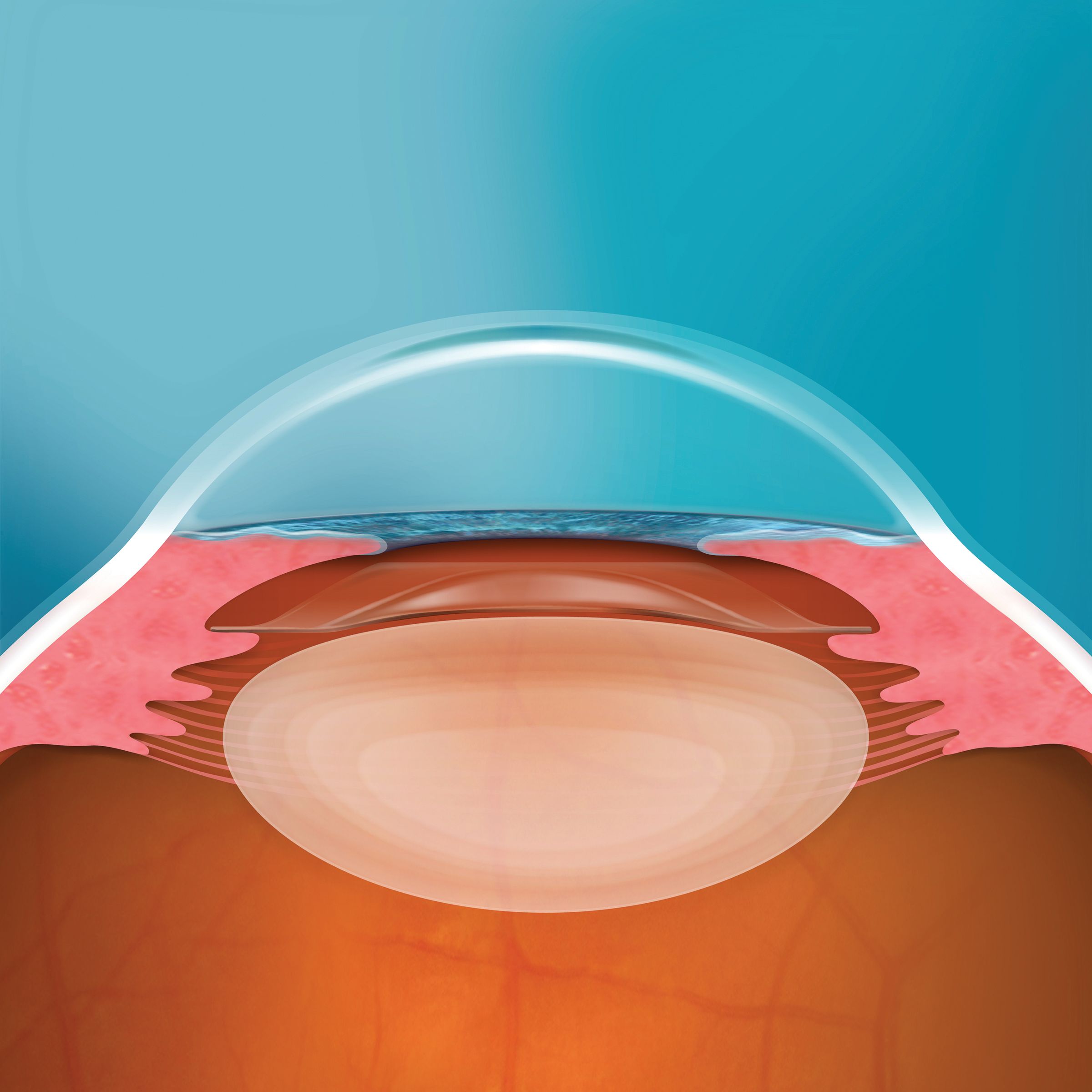
On the other hand, all those options remain open to patients who have undergone phakic IOL implantation. In some of these cases, phakic IOLs can stay in place—eg, when presbyopia is treated with LASIK, blended LASIK, presbyLASIK, or photorefractive keratectomy (PRK). To allow for other presbyopia or cataract treatments, such as replacement of the eye’s natural lens with a multifocal or accommodative lens, doctors can remove phakic IOLs.
Recovery time
Both LASIK and phakic IOLs offer a very quick recovery time, with patients usually seeing 20/20 or better within 24 hours of surgery,
although haziness or light sensitivity may persist a bit longer. Postsurgical discomfort typically lasts 2 to 3 hours after LASIK or phakic IOL implantation.
Although PRK can also be a first choice for treating midrange myopia in younger adults, it comes with a longer recovery period. Full visual acuity accrues over 2 to 4 weeks, and there is a larger amount of discomfort following surgery. For that reason, PRK is not a go-to procedure for most comprehensive refractive surgery practices.
Cost
Phakic IOLs tend to cost about 1.5 times what LASIK does due to the premium material used to manufacture the lenses. However, many patients choose the technology anyway due to its reversibility and the quality of vision they can enjoy after the procedure.
Who are the best candidates for phakic lenses?
The leading phakic IOLs are generally appropriate for patients aged between 21 and 45 years who have myopia ranging from –3 diopters (D) through –20 D. In addition, the lenses can correct vision in patients with up to 4 D of astigmatism.
This means the approach is appropriate for some patients with both myopia and astigmatism who are also candidates for LASIK—as long as they have a large enough anterior chamber depth to accommodate the phakic IOLs.
For some other patients, cornea-altering laser surgeries are contraindicated, making phakic IOLs their only choice. For instance, to avoid an increased risk of lasting adverse effects such as glare, halos, or haze, I avoid performing LASIK in patients with myopia greater than –8 D or PRK in patients with myopia exceeding –6 D.
Other subgroups of patients may be ineligible for LASIK because their corneas are too thin or because they live with persistent dry eye disease, and these are other areas where phakic IOLs shine.
Choosing among phakic IOLs
There are 2 types of phakic IOLs approved by the FDA, and of those, the EVO Visian Intraocular Collamer Lens (ICL) by STAAR Surgical Company is the mainstay across ophthalmology practices.
This lens, which can treat myopia with either a monofocal or a toric design, sits in the posterior chamber, averting the inflammation or damage that can arise from a lens that is affixed to the iris. Made from Collamer, a proprietary, biocompatible collagen copolymer, the EVO ICL lens is well tolerated by the body and, because it is permeable to oxygen, it protects the health of the cornea. Flexible and foldable, the lens enables gentle implantation through a very small incision.
The Artisan Myopia, from Ophtec, which has the distinction of being the first phakic IOL ever approved by the FDA, is an anterior chamber lens that is clipped to the iris. Made of polymethyl methacrylate,3 this lens is not utilized as much anymore in the United States, as its material is less pliable than Collamer, requiring a larger incision and closure using sutures.
Improving client satisfaction
Having used phakic IOLs for nearly 5 years, I appreciate the progress brought to this arena by the FDA’s approval of the EVO ICL in March 2022.4 I have been a subinvestigator in the FDA clinical trial that led to the product’s approval, an experience that allowed me to observe early evidence of its safety and reliability.
In fact, I was so convinced of EVO’s benefits that I later had these ICLs implanted in my sister’s eyes. Along with my other patients who have undergone the procedure, she has joined the ranks of my happiest clients.
With all that we know about the benefits of phakic IOLs, it is imperative that ophthalmologists give more attention to this underutilized technology. I encourage my colleagues to offer implantable ICLs as a first-line choice for younger adults with midrange myopia, providing these patients with the sharpest possible vision while preserving their options for a wide range of refractive treatments as their eyes mature through the full range of ocular milestones.



Brett Mueller II, DO, PhD
e: brett.mueller@muellervision.com
Mueller, the founder of Mueller Vision in Fort Worth, Texas, is a board-certified and fellowship-trained ophthalmologist who has performed thousands of cataract and refractive eye surgeries, including LASIK, laser-assisted lenticule extraction EVO ICL implantation, custom lens replacement, PRK, cataracts, and corneal cross-linking. He is also an associate academic director of the Refractive Surgery Alliance Fellowship Network and has served as a clinical faculty member at the University of the Incarnate Word Rosenberg School of Optometry in San Antonio, Texas. Mueller has received research or consulting support from Alcon, Dompé, Glaukos, Johnson & Johnson, STAAR Surgical Company, and Zeiss in the past year.
References:
Barsam A, Allan BDS. Excimer laser refractive surgery versus phakic intraocular lenses for the correction of moderate to high myopia. Cochrane Database Syst Rev. 2014;2014(6):CD007679. doi:10.1002/14651858.CD007679.pub4
Packer M. Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: six month results from the United States Food and Drug Administration Clinical Trial. Clin Ophthalmol. 2022;16:1541-1553.
Artisan Myopia 204. Ophtec. Accessed January 10, 2024. https://www.ophtec.com/product-overview/artisan-myopia-204
STAAR Surgical announces US FDA approval of EVO Visian Implantable Collamer Lenses. News release. STAAR Surgical Company. March 28, 2022. Accessed January 5, 2024. http://tinyurl.com/2v8ckdyn